Friedman Sue - Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny
Here you can read online Friedman Sue - Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. City: Baltimore, year: 2012, publisher: Johns Hopkins University Press, genre: Home and family. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny
- Author:
- Publisher:Johns Hopkins University Press
- Genre:
- Year:2012
- City:Baltimore
- Rating:5 / 5
- Favourites:Add to favourites
- Your mark:
Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Friedman Sue: author's other books
Who wrote Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny? Find out the surname, the name of the author of the book and a list of all author's works by series.

Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
THE AUTHORS gratefully acknowledge the input, support, and enthusiasm of the many people who helped make this book possible. Thank you to all who shared stories and to each and every one of the healthcare professionals and researchers who took the time to contribute an Expert View.
We appreciate permission to use the filmmakers statement and a quotation from Kartemquin Films In the Family.
A special thanks to those who read and improved what we wrote, including Diljeet Singh, M.D., Susan Domchek, M.D., Minas Chrysopoulo, M.D., Wendy Rubinstein, M.D., Ph.D., Monica Alvarado, M.S., C.G.C., Jana Pruski-Clark, M.S., C.G.C., Rachel Nussbaum, M.S., C.G.C., Tiffani DeMarco, M.S., Sally Scroggs, R.D., L.D., Jennifer Leib, Sc.M., C.G.C., David Winchester, M.D., Amy Fort, Rose Kovatch, Dan Maysey, Barbara Pfeiffer, and Robin Pugh Yi. Ginger Gardner, M.D., graciously provided timely reviews to help us meet deadlines.
And finally, we are indebted to the extraordinary support of Allison Kurian, M.D., Tim Rebbeck, Ph.D., and Victoria Seewaldt, M.D.
SUE FRIEDMAN, D.V.M., gave up her career as a veterinarian to found Facing Our Risk of Cancer Empowered (FORCE), the only national organization dedicated to improving the lives of individuals at high risk for inherited breast and ovarian cancer. Under her direction, FORCE has educated hundreds of thousands of people about the latest advances in cancer prevention, detection, treatment, and related quality-of-life issues. A breast cancer survivor, Sue lives in Florida.
REBECCA SUTPHEN, M.D., F.A.C.M.G., is a board-certified clinical and molecular geneticist with clinical and research expertise in hereditary cancer. She served as director of clinical genetics at Moffitt Cancer Center at the University of South Florida from the programs founding in 1996 until 2009, when she accepted a new role to promote telephone access to board-certified genetics experts as chief medical officer for the countrys largest independent genetic counseling provider, Informed Medical Decisions. She continues her research as a professor in the USF College of Medicine. Rebecca is a member of FORCEs Board of Directors and Medical Advisory Board. A breast cancer survivor, Rebecca lives in Florida.
KATHY STELIGO is a freelance business and health writer. She is the author of The Breast Reconstruction Guidebook and is editor-at-large for FORCE. A two-time breast cancer survivor, Kathy lives in California.
Breast and Ovarian Cancer Basics
FROM A STRICTLY SCIENTIFIC PERSPECTIVE, women have breasts to feed their babies. Yet, for most of us, our breasts are much more than milk-producing glands. Our emotional attachment to our breasts is considerable, increasing as we move from puberty to maturity. Breasts enhance our physical form, give us sexual pleasure, and help us forge a close maternal bond as we nourish our infants. Although our ovaries arent as visible, their reproductive role is more significant, from our first menstrual cycle to monthly fertility and, finally, our change of life. A womans breasts and ovaries are uniquely feminine and intensely personal; the threat of cancer in either is particularly scary.
People with cancer are often surprised if none of their relatives has been diagnosed, but most cancers arent hereditary. The majority are sporadic. They develop from damage that our genes acquire (not inherit) as we age. Genes are fundamental to all living organisms, including humans. They contain instructions for critical body functions and hold all hereditary information that is passed from parent to child. Inherited genetic changes called mutations cause about 5 to 10 percent of breast cancers and 12 percent of ovarian cancers. Most of these hereditary breast and ovarian cancers are caused by mutations in two specific genes, BReast CAncer 1 (BRCA1) and BReast CAncer 2 (BRCA2).raise a womans risk. A family history of breast cancer, even when there is no BRCA mutation in the family, increases breast cancer risk. A strong history of ovarian cancer elevates a womans risk for that disease.
Most breast and ovarian cancers arent hereditary
Sporadic and hereditary cancers differ in important ways that may affect healthcare decisions:
Hereditary cancer often occurs at an earlier age than the sporadic form of the same cancer.
Recommendations for cancer screening and risk reduction can differ, and should begin at a younger age for individuals who have an inherited gene mutation or a family history of cancer.
Multiple family members may inherit the same gene mutation that increases risk for certain hereditary cancers.
Children can inherit a parents gene mutation.
Throughout the remainder of this book, youll learn how inherited mutations or a family history affect your risk for cancer and how you can manage that risk.
More than a million new cases of breast cancer occur each year worldwide. In the United States, its the second most commonly diagnosed cancer (after skin cancer) among women, and it causes more deaths than any other cancer except lung cancer. It also affects men, although far less frequentlyless than 1 percent of all breast cancers occur in men.
Table 1. U.S. breast cancer statistics
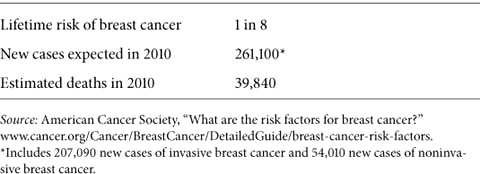
Breast cancer deaths have declined since 1990 because of increased awareness, better methods of early detection, and advances in treatment. Yet too many women, about forty thousand every year, still die from this disease. In the 1970s, a woman living in the United States had a 1 in 11 chance of developing breast cancer in her lifetime; those odds steadily worsened over the next two decades. Since 1999, breast cancer has decreased among women over age 50, while rates among younger women remain unchanged. Today, an average womans lifetime risk of developing breast cancer is 1 in 8 (approximately 12.5 percent) (see ).
Anatomy of the breast
Breast cancer almost always begins in the lobules (the glands that produce milk) or the ducts (the tubes that carry milk to the nipple). Cancer usually develops over several years, typically without pain or other noticeable symptoms, until it shows up as a suspicious calcification on a mammogram or is found as a lump during a breast exam by a woman or her doctor. A tumor may show itself as it grows: a lump or area of thickness, a change in the size or shape of the breast, a skin irritation or dryness that refuses to heal, or unusual tenderness or discharge from the nipple. These same changes often occur with other conditions and dont always signal breast cancer.
Tumors are either in situ, or invasive. In situ, meaning in place, refers to early stage breast cancer that remains within the ducts or the lobules. Nearly all women diagnosed with in situ breast tumors are curedtheir cancer isnt likely to return. Invasive tumors are more worrisome, because if cancerous cells reach the bloodstream or lymph nodes, they can
Font size:
Interval:
Bookmark:
Similar books «Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny»
Look at similar books to Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Confronting hereditary breast and ovarian cancer: identify your risk, understand your options, change your destiny and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.