Jayant - Fast Facts
Here you can read online Jayant - Fast Facts full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2017, publisher: Health Press Limited, genre: Home and family. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Fast Facts
- Author:
- Publisher:Health Press Limited
- Genre:
- Year:2017
- Rating:3 / 5
- Favourites:Add to favourites
- Your mark:
Fast Facts: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Fast Facts" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Jayant: author's other books
Who wrote Fast Facts? Find out the surname, the name of the author of the book and a list of all author's works by series.

Fast Facts — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Fast Facts" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
![]()
| Jayant S VaidyaMBBS MS DNB FRCS PhD FRCS(Gen) Professor of Surgery and Oncology |

| Vivek PatkarMBBS MS MRCS Fellow of European Board of Breast Surgery |

Declaration of Independence
This book is as balanced and as practical as we can make it.
Ideas for improvement are always welcome:
![]()
Fast Facts: Early Breast Cancer
First published January 2017
Text 2017 Jayant S Vaidya and Vivek Patkar
2017 in this edition Health Press Limited
Health Press Limited, Elizabeth House, Queen Street, Abingdon,
Oxford OX14 3LN, UK
Tel: +44 (0)1235 523233
Book orders can be placed by telephone or via the website.
To order via the website, please go to: fastfacts.com
For telephone orders, please call +44 (0)1752 202301.
Fast Facts is a trademark of Health Press Limited.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the express permission of the publisher.
The rights of Jayant S Vaidya and Vivek Patkar to be identified as the authors of this work have been asserted in accordance with the Copyright, Designs & Patents Act 1988 Sections 77 and 78.
The publisher and the authors have made every effort to ensure the accuracy of this book, but cannot accept responsibility for any errors or omissions.
For all drugs, please consult the product labeling approved in your country for prescribing information.
Registered names, trademarks, etc. used in this book, even when not marked as such, are not to be considered unprotected by law.
A CIP catalogue record for this title is available from the British Library.
ISBN 978-1-910797-12-9
eISBN 978-1-910797-24-2
Vaidya JS (Jayant)
Fast Facts Breast Cancer/
Jayant S Vaidya, Vivek Patkar
The authors wish to thank Professor David Joseph, Dr Alison Jones, Professor Michael Baum and Professor Harvey Schipper for their contributions to previous editions of Fast Facts: Breast Cancer from which some of this text is adapted: Vaidya JS, Joseph D. Fast Facts: Breast Cancer, 5th edn. Oxford: Health Press Limited, 2014.
Medical illustrations by Dee McLean, London, and
Anna-Maria Dutto, Withernsea, UK.
Printed in the UK with Xpedient Print.
In developed countries, breast cancer is usually diagnosed at an early stage when it is still confined to the breast and regional nodes. Here, we focus on stage 0 (ductal carcinoma in situ), I, II and IIIA disease, with a concise overview that will aid understanding of the risk of developing breast cancer, the essentials of diagnosis and preoperative assessment and the current approach to treatment and follow-up.
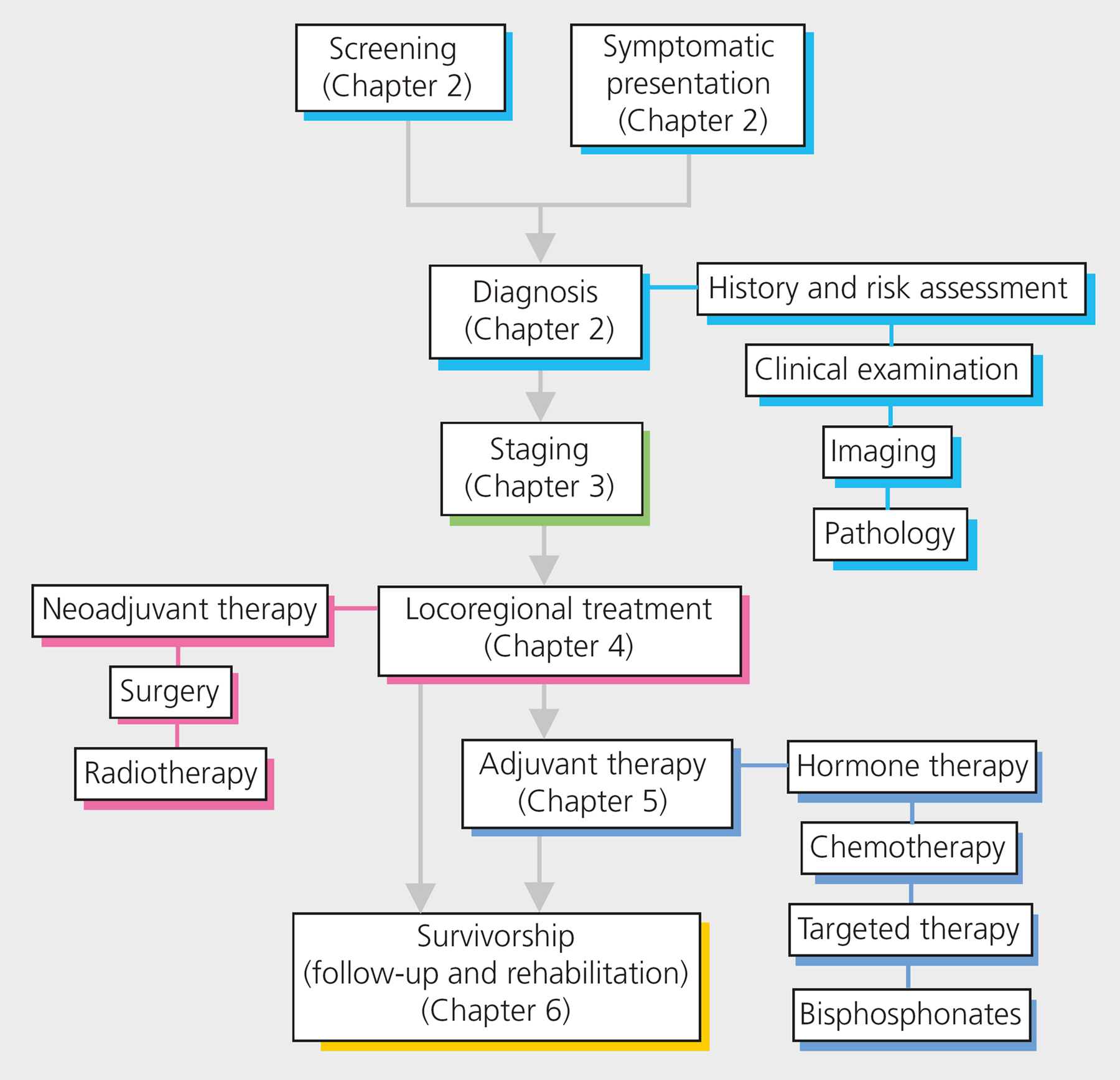
Use Fast Facts: Early Breast Cancer to follow clear diagnostic and treatment pathways, from screening and symptomatic presentation, through triple assessment diagnosis, to treatment and follow-up.
Early breast cancer refers to cancer that has not spread beyond the breast or the axillary lymph nodes. This includes ductal carcinoma in situ (DCIS; stage 0) and stage I, IIA, IIB and IIIA invasive breast cancers (see ). The term invasive is unique to breast cancer: in no other cancer is such tautology used. It simply means that cancer cells have crossed the basement membrane of the duct and can potentially spread. It is only used because of the popularity of the terms ductal or lobular carcinoma in situ (DCIS and LCIS) in which cancer cells have not crossed the basement membrane; such lesions, if pure, are theoretically not a risk to life. DCIS and LCIS are most commonly identified by mammographic screening or as a chance finding after a biopsy of a benign lesion. Ductal intraepithelial neoplasia (DIN) would be the preferred name and would remove the unnecessary taboo of cancer when these lesions are diagnosed.
There are no histopathological or molecular markers to predict the progression from DCIS to invasive disease with certainty. However, the risk of invasive cancer is believed to be increased by nine- to elevenfold in a woman in whom DCIS is treated by removal of the affected area alone.
Breast cancer is the most common form of cancer among women, with an estimated 1.67 million new cases diagnosed worldwide in 2012.
The breast is composed of glandular and adipose tissue in varying proportions. The glandular tissue consists of 1520 lobes containing numerous lobules, linked by ductules (). The ductules combine to form the lactiferous ducts, which open into the lactiferous sinuses and empty through the nipple. The breast is enclosed in two layers of fibrous tissue connected by Coopers ligaments, which give it its characteristic shape. Invasion of Coopers ligaments by cancer and cicatrization shortens the ligaments, leading to the classic early sign of dimpling of skin when the pectoralis is contracted or when the patient has their arms raised when bent forward.
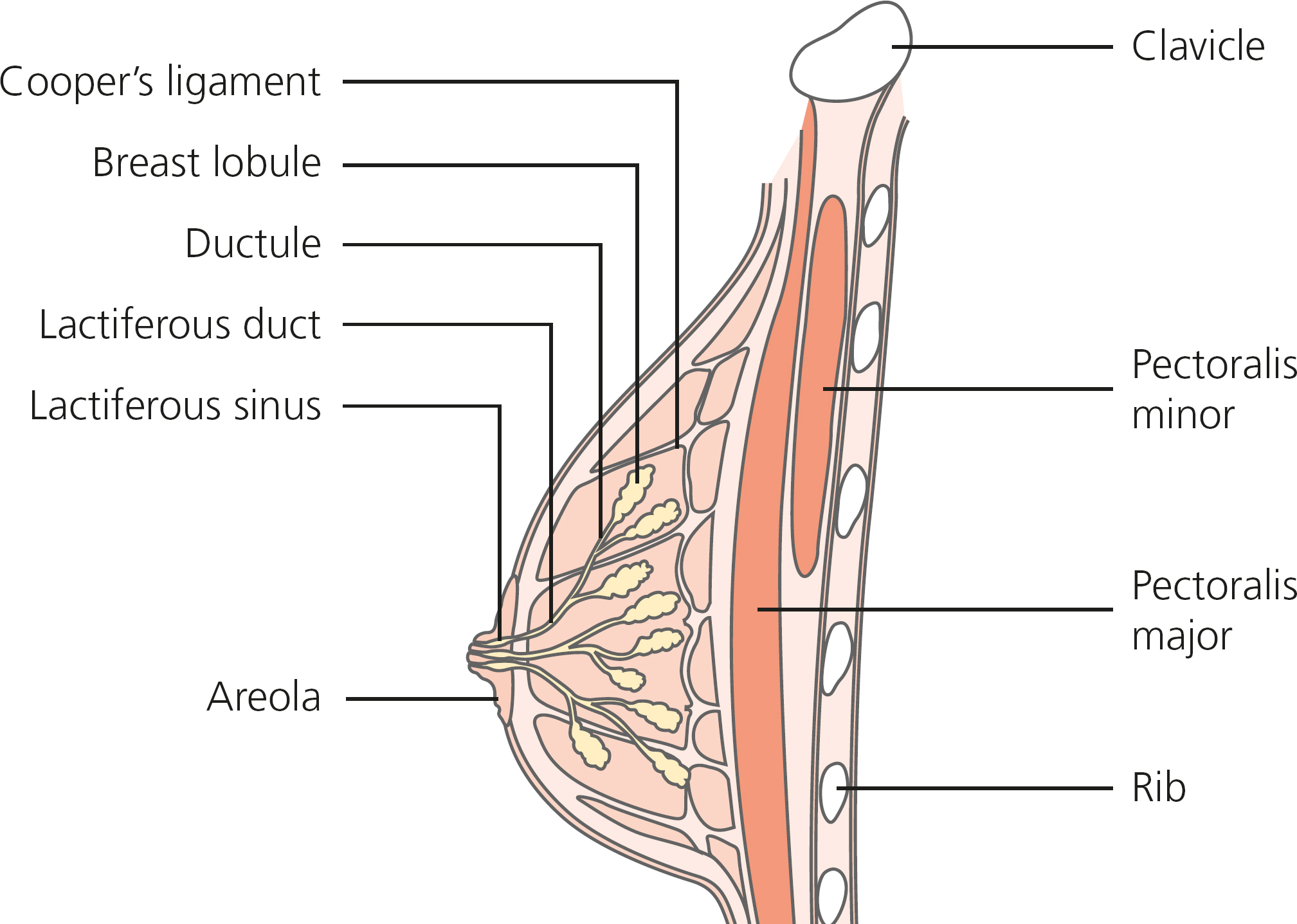
Figure 1.1 Structure of the normal breast.
The lymphatics of the breast tissue converge in the subareolar plexus of Sappy, and then drain into the axilla (armpit).
Most breast cancers are epithelial tumors, arising from either the milk-producing glands (lobular carcinomas) or, more commonly, from the draining ducts (ductal carcinomas); only a small number are non-epithelial involving the stroma or soft tissues.
Ductal carcinomas account for over 90% of breast cancers. Lobular carcinomas account for approximately 8% of breast cancers. Such tumors may occur at several sites, either in the same breast or in both breasts. They can be hard to diagnose, as their diffuse nature and relative radiolucency mean that they often do not show up on mammograms.
Phyllodes tumors are relatively rare stromal tumors that only very rarely exhibit the malignant features of a true sarcoma. Clinically and on imaging they resemble fibroadenomas, although they are often larger.
Receptor status. Estrogen and progesterone are important regulators of normal breast growth and development and play important roles in the pathogenesis of breast cancer. The hormone receptors in some breast cancers promote DNA replication and cell division when estrogen or progesterone bind to them (e.g. an estrogen-receptor positive [ER+] tumor), while the presence of the receptor for human epidermal growth factor 2 (HER2) correlates with a poorer prognosis at any given stage of cancer. These receptors provide valuable therapeutic targets, as blocking them can stop cancer growth and may even lead to complete regression.
Next pageFont size:
Interval:
Bookmark:
Similar books «Fast Facts»
Look at similar books to Fast Facts. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Fast Facts and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.