Lawton Luke - Own the Arterial Blood Gas
Here you can read online Lawton Luke - Own the Arterial Blood Gas full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2016, publisher: CALL the Doctors Publishing, genre: Home and family. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
- Book:Own the Arterial Blood Gas
- Author:
- Publisher:CALL the Doctors Publishing
- Genre:
- Year:2016
- Rating:4 / 5
- Favourites:Add to favourites
- Your mark:
Own the Arterial Blood Gas: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Own the Arterial Blood Gas" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Lawton Luke: author's other books
Who wrote Own the Arterial Blood Gas? Find out the surname, the name of the author of the book and a list of all author's works by series.

Own the Arterial Blood Gas — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Own the Arterial Blood Gas" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
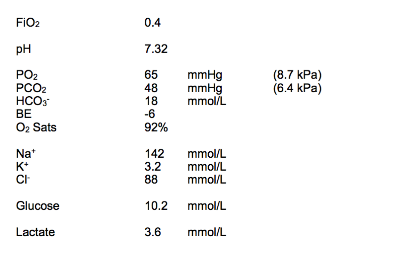
No compensation. 2. Oxygenation Critical hypoxia on supplemental oxygen. A-a gradient in mmHg for FiO 40% = 300 (1.25 x 48) 65 = 300 60 65 = 300 = 175 Grossly elevated ! (expect for 26yo female = 26/4 + 4 = ~10) Gross V/Q mismatch Implies critical/life threatening asthma Also consider : ARDS (SIRS/aspiration) , i nterstitial lung disease , o ther respiratory membrane disease (eg LRTI) , PE A-a gradient in mmHg for FiO 40% = 40 kPa (1.25 x 6.4) 8.7 = 40 8 8.7 = 23.3 kPa 3. Electrolytes Normonatraemia Mild hypokalaemia Possible intracellular shift if using salbutamol Expect K + for pH = 5 + 0.5 x 5 = 5.25 mmol/L Therefore significantly K + deficient on correction Replace K + and monitor ECG Normochloraemia Moderate hyperglycaemia Secondary to glucocorticoid administration Possible diabetes check medical Hx Moderate hyperlactataemia Likely due to salbutamol administration (B ) Type A less likely with normal haemodynamics Type B less likely with N temperature, but evaluate for sepsis 4. Interpret **This is a critically ill patient*** Asthmatic, and ABG shows the dual processes of r espiratory acidosis and RAGMA Respiratory acidosis VERY concerning given Hx of asthma Indicates critical/life threatening disease Hypercapnoeic asthma often precedes respiratory arrest Needs urgent treatment High dose bronchodilators, MgSO , CPAP, possible IPPV Involve intensive care service RAGMA , h yperlactataemic Salbutamol Sepsis/shock less likely Check to exclude other drug causes (Iron, isoniazid, paraldehyde, toxic alcohols, metformin etc) Also consider other causes Diabetic ketoacidosis (h yperglycemic ) : check med Hx and urine/blood ketones Uraemia : c heck renal function
She has been treated by her GP for 2 days with bronchodilators and glucocorticoids . The stem again provides valuable information. This is a high risk patient , and candidates will need to add perspective to their answer. Usually asthmatics present with hyperventilatory hypocapnoea. Here the presence of hypercarbia indicates severe asthma, and a PEFR <25% of the patients norm . Respiratory collapse is imminent.
This is underlined by a comment during the evaluation of the A-a gradient to show the candidates understanding of severity. Several minor issues require comment in this blood gas, including the presence of a significant K + deficit, hyperglycaemia (presumably related to steroids) and hyperlactataemia (salbutamol therapy). Again these are included in the main body of working, so that the interpretation phase can be focused on the major issues. Critically, in the interpretation phase the candidate must highlight the importance of the presentation. Phrases such as this is a critically ill patient are useful in this instance. An overview of relevant treatment is indicated.
A full differential for the RAGMA can also be included should time allow.
Dhuper S, Maggiore D, Chung V and Shim C. Profile of near-fatal asthma in an inner-city hospital. Chest 2003; 124 (5): 1880-84 Martin TG, Elenbaas RM and Pingleton SH. Use of peak expiratory flow rates to eliminate unnecessary arterial blood gases in acute asthma. Ann Emerg Med 1982 11(2):70
Acid base status Mild alkalaemia Normocapnoea Moderately elevated HCO - : m etabolic alkalosis expect CO = 20 + (0.7 x 32) = 20 + 21 = 42 mmHg therefore CO is appropriate compensation AG/DR not applicable for met alkalosis Therefore diagnose primary metabolic alkalosis with appropriate respiratory compensation. 2. Oxygenation Venous sample, therefore A-a gradient not applicable 3. Electrolytes Normonatraemia Normokalaemia Expect K + for pH = 5 - (1 x 0.5) = 4.5 mmol/L Therefore K + is roughly pH appropriate Normochloraemia Significant hypercalcaemia Moderate hypophosphataemia Elevated renal indices U:C ratio ~90 Likely pre-renal Assess volume status Check medication history for contributors (ACEi/frusemide) 4. Interpret VBG shows m etabolic alkalosis with appropriate respiratory compensation Marked hypercalcaemia and hypophosphataemia Renal failure Given clinical history this suggests Milk-Alkali Sx as a complication of long term Ca 2+ therapy Treat IV fluids, monitor Ca 2+ , consider diuretics/bisphosphonates Cease Ca 2+ supplements Check ECG for QT prolongation Other causes of high Ca 2+ : Primary hyperparathyroidism Metastatic Ca/myeloma ?pathologic fracture: evaluate xrays Other causes alkalosis: Endocrinopathies : Cushings Sx (less likely due to N electrolytes) , Bartter s Sx Loop diuretics (unlikely with increased Ca/K) HCl loss : c larify if any vomiting COMMENTS An 85 year old female presents with a left hip fracture . She has been on long term calcium and vitamin D supplements as osteoporosis prophylaxis.
A venous blood gas is taken and the results are shown below. This stem again represents an unusual cue to an acid base disturbance, and candidates may wish to proceed first by systematically working the question. Doing so reveals a metabolic alkalosis complicated by hypercalcaemia and renal failure. This is the milk-alkali syndrome, caused by large amounts of calcium and ingestible alkali. Historically it was associated with milk and sodium bicarbonate treatment for peptic ulcer disease, but today is prevalent as a complication of the widespread use of calcium carbonate for osteoporosis prophylaxis .
Picolos MK, Lavis VR and Orlander PR.
Picolos MK, Lavis VR and Orlander PR.
Milk-alkali syndrome is a major cause of hypercalcaemia among non-end-stage renal disease (non-ESRD) inpatients. Clin Endocrinol 2005; 63(5): 566 - 76
- HR: 112 /min
- BP: 99/62 mmHg
- RR: 34 /min
- Sats: 100% RA
- T: 37.8 o C
- GCS:
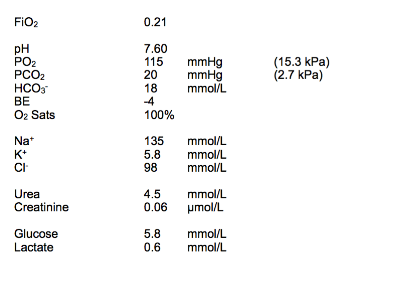
Acid base status Profound alkalaemia Profound hypocapnoea : r espiratory alkalosis Expect HCO - for CO Acute = 24 - (2 x 2) = 20mmHg Chronic = 24 - 2 x 5 = 14mmHg Mild decrease in HCO - : m etabolic acidosis Not consistent with either acute or chronic compensation for CO Anion Gap = 135 18 98 = 135 = 19 RAGMA Delta Ratio = (19-12) /( 24-18) = 7/6 = ~1 Implies isolated RAGMA Therefore diagnose: acute respiratory alkalosis metabolic acidosi s: partly compensation / partly RAGMA 2. Oxygenation Hyperoxaemia on RA Secondary to gross hyperventilation Implies central respiratory stimulation A-a gradient in mmHg FiO 21% = 150 (1.25 x 20) 115 = 150 25 115 = 150 = 10 Expect A-a gradient 30yo female = 30/4 + 4 = 7.5 + 4 = 11.5 Not elevated No V/Q mismatch A-a gradient in kPa FiO 21% = 21 kPa (1.25 x 2.7) 15.3 = 21 3.38 15.3 = 2.32 kPa 3. Electrolytes Normonatraemia Not cause of confusion Mild hyperkalaemia Expect K + for pH = 5 - 2 x 0.5 = 4.0 mmol/L K + level elevated when corrected for pH Monitor telemetry as pH corrected Mild hypochloraemia Renal equilibration for RAGMA Normoglycaemia Not cause for decreased GCS/confusion DKA unlikely Normal lactate Not cause for RAGMA Normal renal indices Not cause for RAGMA 4. Interpret ABG shows a cute primary respiratory alkalosis with hyperoxaemia and some metabolic compensation and concurrent RAGMA . Primary respiratory alkalosis in absence of hypoxia implies central respiratory stimulation Most consistent with Aspirin overdose, given clinical Hx Also fits with RAGMA (N lactate and urea) Mx: A lkalini ze urine and IV fluid load Serial salicylate levels to Ax therapy Check paracetamol level (co-ingestant) Consult toxicology Psychiatry input RE suicide attempt
Font size:
Interval:
Bookmark:
Similar books «Own the Arterial Blood Gas»
Look at similar books to Own the Arterial Blood Gas. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Own the Arterial Blood Gas and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.