Bob Mash - Handbook of Family Medicine
Here you can read online Bob Mash - Handbook of Family Medicine full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2018, publisher: Oxford University Press, genre: Science. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
Handbook of Family Medicine: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Handbook of Family Medicine" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Bob Mash: author's other books
Who wrote Handbook of Family Medicine? Find out the surname, the name of the author of the book and a list of all author's works by series.



Handbook of Family Medicine — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Handbook of Family Medicine" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Bob Mash, Khaya Mfenyana
The establishment of family medicine as an academic discipline provides a context of learning that is different from that of the traditional teaching hospital. In South Africa, as in many other countries, it is now considered essential to train doctors not only in the traditional academic teaching hospital but also in the district health system, within clinics, health centres and district hospitals. This is to allow medical students to deal with the common problems encountered in all types of settings. If medical students were only exposed to academic teaching hospitals their experience of and preparation for handling typical health problems would be significantly limited. Figure 1.1 shows, during a typical month in the USA, that less than one person in 1 000 is admitted to a teaching hospital, while 217 people consult a doctor elsewhere. This chapter is intended to describe this different context of care and help the student to understand how this context differs from the traditional teaching hospital.
In this chapter, we refer to personal experience of the contexts in which we work. Professor Khaya Mfenyana has worked in rural clinics in the Eastern Cape and Professor Bob Mash in Khayelitsha, a large peri-urban township outside Cape Town. The majority of their patients are poor, use the public health sector, and speak Xhosa as their first language.
Recent work in South Africa has defined the burden of disease in our communities (Bradshaw, 2007). The burden of disease is defined in terms of years of life lost due to premature death or disability (sometimes referred to as disability adjusted life years or DALYs). Figure 1.2 and Table 1.1 show the top 20 conditions that cause the greatest burden of disease in South Africa. These conditions can be categorised into four broad groups:
Conditions related to HIV and Aids (such as TB)
Conditions related to violence and trauma (such as interpersonal violence, intimate partner violence and road traffic accidents)
Conditions related to chronic non-communicable diseases (such as hypertension, diabetes, heart disease, asthma)
Conditions related to maternal and child health (such as pregnancy induced hypertension, post-partum haemorrhage, pneumonia, diarrhoea and low birth weight).
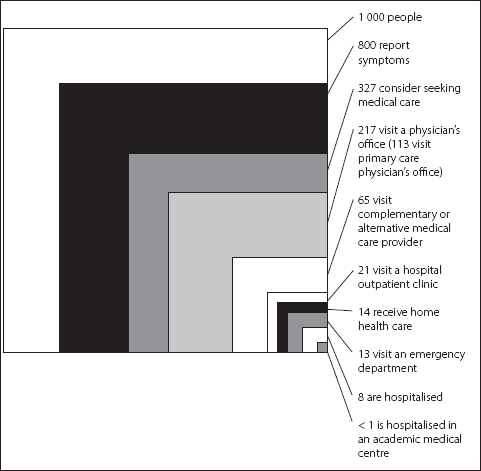
Figure 1.1 The ecology of medical care
NOTE: Each box contains a subgroup of the biggest box of 1 000 persons
Source: Green L, Fryer G, Yawn B, Lanier D, Dovey S (2001) The Ecology of Medical Care Revisited N Engl J Med 344: 20212025. [Online]. Available at: DOI: 10.1056/NEJM200106283442611
South Africa is often said to have a quadruple burden of disease; conditions related to poverty and under-development are often combined with conditions related to the transition to a more urbanised and developed society.
Underlying this burden of disease are a variety of risk factors, which have been identified (see Table 1.1) and knowing these risk factors gives us the opportunity to prevent these common conditions. Unsafe sex, interpersonal violence, alcohol abuse and smoking tobacco make up the top four risk factors. Interestingly, being overweight and underweight are both listed sequentially as important risk factors. Disease prevention and health promotion are discussed further in Chapter 4.
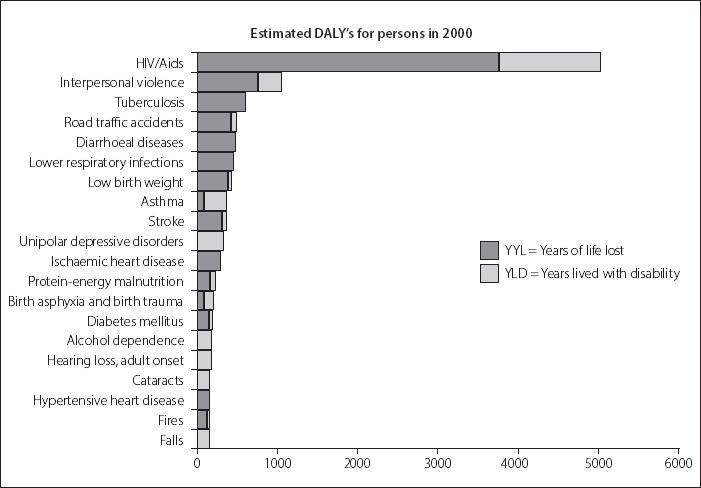
Figure 1.2 The burden of disease in South Africa
Source: Bradshaw D, Norman R, Schneider M (2007) A clarion call for action based on refined DALY estimates for South Africa. S Afr Med J June, 97(6): 438, 440
Table 1.1 Risk factors and the burden of disease in South Africa
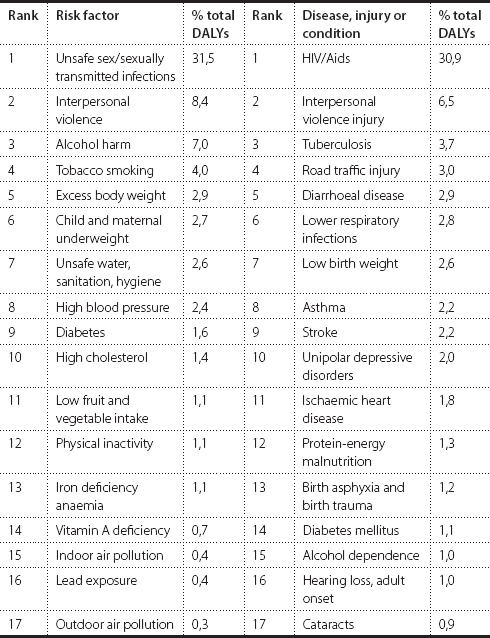
Source: Norman, R et al (2007) A comparative risk assessment for South Africa in 2000: Towards promoting health and preventing disease. South African Medical Journal 97(8): 637. [Online]. Available at: http://www.samj.org.za/index.php/samj/article/view/654/151 (Accessed: 10 January 2017)
The burden of disease discussed above may present in a wide variety of ways at the primary care level. Table 1.2 shows the most common symptoms with which people present to ambulatory primary care in South Africa (Mash, Fairall et al., 2012). These are derived from a study of 19 000 consultations spread across the Western Cape, Northern Cape, North West and Limpopo provinces. Primary care providers must have an approach to the assessment of all these symptoms. South African primary care differs from other countries in America, Asia and Europe in the frequency of generalised body pain as a complaint and in the frequency of symptoms that are probably due to HIV/Aids and TB (weight loss, sweating, loss of appetite, abnormal sputum, respiratory pain and dysphagia) or STIs (genital/pelvic pain, vaginal and urethral discharge and vaginal symptoms).
Cough is usually a symptom of upper respiratory tract infection and this disease is usually self limiting. However, it is a challenge for the family physician not to take things lightly, as cough may be a symptom of a serious disease. The history and physical examination therefore become very important. Could this be pneumonia, tuberculosis, asthma, or cardiac failure, for example?
Headache is a common symptom that can easily be ignored and yet can be a pointer to a serious underlying problem, either psychological or organic. In our context, many patients who say Doctor, I have a headache are indirectly saying Doctor, can you check my blood pressure? Unfortunately, many headaches tend to be associated with hypertension, not because headaches per se are a common symptom of hypertension, but because many hypertensive patients have tension headaches. So, while tension headaches should be diagnosed and treated appropriately, it is the real reason for the headache that is important.
Fever is another common presenting problem. In our context, patients may complain of fever, but when asked what exactly they mean or what they feel, several answers may come up. These may include ubushushu (hotness), or umkhuhlane (a common cold), or ingqele (cold), or ubugxathu (pain between the shoulders). When we examine these patients, we may find that they have an upper respiratory tract infection and/or an elevated temperature, or no signs at all. Ingqele does not always imply an upper respiratory tract infection. The patient may have a serious illness characterised by fever and rigors, but, on the other hand, the patient may have no signs of any disease or may just have pain between the shoulders. Ingqele may be attributed to a certain day when the patient was exposed to rainy or cold weather and this day may not be yesterday or last week. Pain between the shoulders may also be attributed to stress or heavy manual work. Therefore it is always important to find out what the patient thinks about the illness. The other interesting symptom we are picking up in our environment is painful throbbing neck veins. This is usually related to stress.
Abdominal pain is another common symptom, which may be a symptom of conditions such as gastritis, pelvic inflammatory disease, cystitis and so on. Some patients will describe feeling as if something is going up from the abdomen to the chest. Some will talk of umoya oshushu onyukayo (hot wind that is going up). These are examples of ill-defined symptoms that can only be left at a symptom level at this stage of our understanding, as putting a diagnostic label on them would be premature, irrelevant, and dangerous. What would be more helpful would be to try to understand what that particular patient means by their description of the symptom. We need to explore patients thoughts, feelings, beliefs, and expectations carefully in order to unearth the real reason for encounter. If, on the other hand, the feeling that something is going up from the abdomen to the chest is summarised as abdominal pain, there is a danger of reducing the whole interview to only the routine questions of Is it colicky in nature?, Does it radiate?, What relieves it?, and so on. Understanding the culture and language of the people you are serving is helpful in these situations.
Next pageFont size:
Interval:
Bookmark:
Similar books «Handbook of Family Medicine»
Look at similar books to Handbook of Family Medicine. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Handbook of Family Medicine and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.