Meechan - Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6
Here you can read online Meechan - Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6 full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2010, publisher: Quintessenz Verlag, genre: Children. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Meechan: author's other books
Who wrote Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6? Find out the surname, the name of the author of the book and a list of all author's works by series.


Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6 — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Quintessentials of Dental Practice 6
Oral Surgery and Oral Medicine 1
Quintessence Publishing Co. Ltd.
British Library Cataloguing in Publication Data
Meechan, J. G.
Practical dental local anaesthesia. - (The quintessentials of dental practice)
1. Anesthesia in dentistry 2. Local anesthesia
I. Title II. Wilson, Nairn H. F.
617.9'676
ISBN 1-85097-325-3
Copyright 2002 Quintessence Publishing Co. Ltd., London
All rights reserved. This book or any part thereof may not be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, or otherwise, without the written permission of the publisher.
ISBN 1-85097-325-3
Painless, effective local anaesthesia is a real practice builder. Irrespective of how confident prospective readers may be about their knowledge and techniques in dental local anaesthesia, this volume in the Quintessentials for General Dental Practitioners Series is bound to provide new knowledge and understanding. Questions as to what best to do, where and when, notably in the presence of complicating factors and in the event of failed anaesthesia, are addressed in confidence-giving detail. The text, in the style of the Quintessentials Series, has been prepared primarily for the hard-pressed practitioner and the student seeking the benefit of experience tempered by authoritative insight.
Practical Dental Local Anaesthesia will give practitioners and students alike something to apply for the immediate benefit of their patients. Whether this benefit stems from a nugget of information or a stimulus to adopt a fresh approach to state-of-the-art dental local anaesthesia, Practical Dental Local Anaesthesia will undoubtedly prove to be a valuable addition to every dentists library.
Nairn Wilson
Editor-in-Chief
This book could not have been written without the help of a number of people. Janet Howarth, Jan Ledvinka, Carole Rose and David Rynn all helped with the photography in Newcastle. John Rout of the Birmingham Dental Hospital kindly provided Fig 9-1. Figs 7-1 and 9-4 are reproduced from Dental Update by permission of George Warman Publications (UK) Ltd. Fig 9-5 originally appeared in R R Welbury (ed.), Paediatric Dentistry, and is reproduced by permission of Oxford University Press.
The time invested in writing this book would not have been possible without the understanding and support of my family. So to Jan, Rob and Si a big Thank you.
John G Meechan
The aim of this chapter is to describe the basic principles of dental local anaesthesia.
After reading this chapter you should have a basic understanding of the pharmacology and anatomy of dental local anaesthesia.
The main purpose of this book is to act as a practical guide to the use of local anaesthesia in dentistry. Before embarking on practical issues it is important to acquire a basic understanding of the pharmacology and anatomy of dental local anaesthesia. Anaesthesia is defined as a loss of sensation in a circumscribed area of the body by a depression of excitation in nerve endings or an inhibition of the conduction process in peripheral nerves. This definition includes all sensation. In dentistry it is pain sensation we want to eliminate. Loss of pain sensation is termed analgesia. The terms local anaesthesia and local analgesia are used almost synonymously in dental practice. As true anaesthesia may be produced on occasion following intra-oral injection, the former term is used in this book.
Local anaesthesia may be obtained by a number of mechanisms. Traumatic severance of a nerve will produce it. This may occur after damage to the lingual nerve during third molar surgery. This is not always reversible. In order to be acceptable for clinical use a reversible method is required. Local anaesthetic drugs achieve this goal. Although the mechanism of local anaesthetic action is complex it can be explained in a straightforward way. A nerve transmits information along its length by producing a change in the electrical gradient across the nerve cell membrane (Fig 1-1). At rest the inside of the nerve cell is negatively charged compared to the outside. When the nerve is excited to the so-called firing level this polarity changes. The reversal in electrical charge is the signal that is transmitted along the nerve. This change in polarity is principally due to the rapid entry of positively charged sodium ions into the cell. At rest the cell is impermeable to sodium ions. Stimulation causes a conformational change that permits the inward passage of these positive ions. Thus, transmission is dependent upon sodium ion entry. This occurs at the sodium channel. Local anaesthetics work by inhibiting the passage of sodium into the nerve cell. In simple terms they act as chemical roadblocks to the transmission of electrical impulses. They achieve this by a combination of two mechanisms. First, there is probably a contribution to the effect by a non-specific expansion of the nerve cell membrane. This causes physical obstruction of the sodium channel. Secondly, and more importantly, local anaesthetics bind reversibly to specific receptors in the sodium channel. The binding site for the local anaesthetic molecule is exposed during a conformational change that occurs to the sodium channel during the refractory period of the firing cycle. During this period further stimulation of the nerve is ineffective in producing a signal. When the local anaesthetic binds to its receptor the sodium channel is maintained in the refractory conformation. A simplified diagrammatic representation of this action is shown in Fig 1-2.
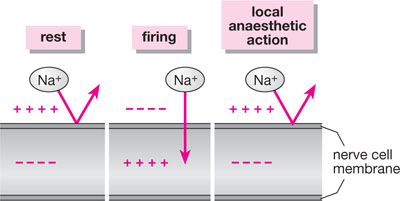
Fig 1-1 The major factor involved in nerve transmission is the differential concentration of sodium ions across the nerve membrane. Local anaesthetics block the entry of sodium into the cell and thus prevent firing.
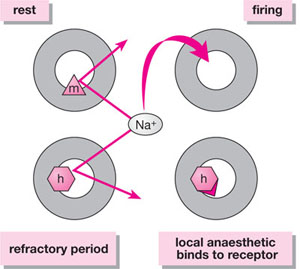
Fig 1-2 At rest, ion passage through the sodium channel is inhibited by a gate known as the m (for make) gate. This gate is open during firing. During the refractory period, another gate, the h (for halt) gate, closes blocking further sodium entry. The local anaesthetic molecule binds to a receptor on or close to the h gate maintaining the channel in the refractory conformation.
Access to the local anaesthetic binding site is obtained from the inside of the nerve cell. This is important and represents an interesting pharmacological challenge. Why? In order to gain entry into the cell the anaesthetic must be soluble in fat, as the cell membrane contains much lipid. Non-charged molecules are fat-soluble. Therefore, to gain entry into the cell the local anaesthetic must be in a non-charged state. As specific binding to a receptor is important in achieving anaesthesia a material that recognises its receptor is needed. Receptor binding depends upon the molecule being charged. Thus, once in the cell, it is important that the molecule is in a charged form. This ability to exist in both lipid-soluble and charged states is achieved because local anaesthetics are weak bases. When the local anaesthetic is in solution some of the molecules are charged and some are uncharged (Fig 1-3). It is only the uncharged molecules that can penetrate the lipid nerve cell membrane to gain access to the inside of the cell. The uncharged portion enters the nerve cell and then re-equilibrates in this aqueous environment to a mixture of charged and uncharged molecules. Once in the cell it is the charged portion that binds to the specific receptor. If no material enters the cell the local anaesthetic will not function. The more rapidly a local anaesthetic enters the cell the more effective it is and the quicker it will act. Thus materials that have a high proportion of uncharged molecules present in tissue fluid after injection are the most effective. Two factors govern the proportion of charged to uncharged molecules following injection. These are:
Next pageFont size:
Interval:
Bookmark:
Similar books «Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6»
Look at similar books to Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Practical Dental Local Anaesthesia: QuintEssentials of Dental Practice Vol. 6 and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.