Springer International Publishing Switzerland 2016
Jean-Franois Bonneville , Fabrice Bonneville , Franoise Cattin and Sonia Nagi MRI of the Pituitary Gland 10.1007/978-3-319-29043-0_1
1. MRI Technique and Radiological Anatomy of the Pituitary Gland
1.1 Basic MRI Sequences
Three basic sequences are indicated in all clinical situations. These sequences are often adequate for the diagnosis, particularly in the search for microprolactinomas. Additional sequences may be obtained according to the clinical and biological status and after reading the basic sequences.
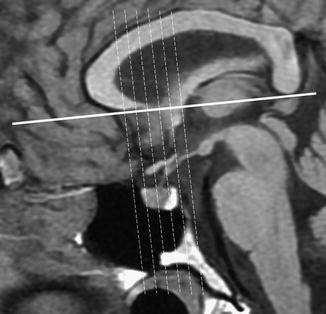
Sagittal T1W sequence focused on the pituitary region constitutes the first step of the MR examination: this sequence is rarely informative in the diagnosis of intrasellar lesions, but allows one to draw an anatomical plane, for example the sub-callosal plane, which will allow perfect reproducibility of the coronal cuts for serial MRI (Fig. ).
Fig. 1.1
Sagittal T1WI. The coronal cuts are obtained perpendicularly to the sub-callosal plane
Fig. 1.2
Normal pituitary gland. ( a , b ) Sagittal T1 and CE T1WIs. ( c , d ) Coronal T1 and T2 WIs at the anterior part of the pituitary gland. ( e , f ) Coronal T1 and T2 WIs, 2 mm posterior to ( c ) and ( d ). Anterior lobe ( curved arrow ). Posterior lobe ( thick arrow ). Pituitary stalk ( thin arrow ). On T2WI, a flow artifact in the suprasellar cistern blurs the pituitary stalk. Optic chiasm ( asterisk ). After gadolinium injection ( b ), enhancement of anterior lobe, pituitary stalk, and tuber cinereum ( open arrow )
When an intrasellar lesion is suspected on the sequences without contrast, the diagnosis can be confirmed by the realization of coronal T1WI after gadolinium injection (CE T1WI). A low dose of contrast medium (0.05 mmol/k) is recommended to avoid a too intense enhancement, which may hide a small intraglandular lesion. Nevertheless, it is our own policy to spare gadolinium administration when the clinical situation is clear and confirmed by the noncontrast T1 and T2WI, for instance when searching for microprolactinomas. Delayed imaging 45 min after gadolinium injection can have some interest, mainly in Cushing disease, in revealing a very small microadenoma (picoadenoma) when T1, T2, and CE T1WI are not informative.
In the case of a lesion with suprasellar extension, coronal and sagittal T1W sequence after gadolinium injection and, if necessary, a 3D gradient echo T1W acquisition with gadolinium for neurosurgical planning are performed.
1.2 Additional Sequences
Axial TWI, preferentially with fat saturation is the best sequence to evaluate the storage of vasopressin and is thus highly recommended for the exploration of diabetes insipidus. This sequence will also be extremely useful to consolidate the diagnosis of intrasellar Rathke cleft cyst even when associated with pituitary microadenoma.
In the exploration of Cushing disease, if the standard sequences including the sequences after gadolinium injection are negative, a dynamic imaging is obtained (Fig. ). A 3D T1W gradient-echo sequence with inframillimetric section thickness may demonstrate a tiny ACTH-secreting pituitary microadenoma.
Fig. 1.3
Dynamic MRI of the normal pituitary gland. ( a ) Before contrast injection. ( b ) About 30 s later, opacification of the pituitary stalk and the secondary capillary bed ( arrow ). ( c ) At 60 s, the enhancement of the pituitary gland is intense and homogeneous. ( d f ) Slow decrease of enhancement intensity
3D TOF MRA is useful in the lesions affecting the cavernous sinus, particularly in the diagnosis of aneurysm of the intracavernous internal carotid artery, ectasic carotid siphons, and dural fistula, or to confirm anatomical variations such as persistent trigeminal artery.
1.3 Advanced MRI Techniques
Diffusion imaging, perfusion imaging, and proton MR spectroscopy (MRs) can be helpful in differentiating various types of lesions involving pituitary gland and hypothalamus. These techniques require the positioning of a region of interest (ROI) with a sufficient size, and thus may have a role only in the evaluation of large lesions.
Diffusion imaging can have an interest in early detection of pituitary infarction or pituitary apoplexy and in differentiation of abscess from hemorrhage, the ADC value being considerably decreased in pituitary ischemia and abscess. The relationship between diffusion imaging and apparent diffusion coefficient on one hand, and consistency of the pituitary adenoma on the other, is controversial. For some authors, macroadenomas with hypersignal on diffusion imaging and a low ADC value present a soft consistency, while those with hyposignal and a high ADC value are firmer: these data may have been useful for the neurosurgeon but are not confirmed in recent studies. It is generally admitted today that there is no correlation between the ADC and both the consistency and secretory type of the pituitary adenoma.
MRs has a limited interest in the diagnosis of pituitary lesions. However, some MRs patterns can help to confirm a diagnosis evoked on standard sequences. Hypothalamic gliomas demonstrate increased choline peak and decreased N-acetylaspartate (NAA) peak. In craniopharyngiomas and germinomas, a high level of lipids is usually observed with only some traces of other metabolites. Hypothalamic hamartomas are characterized by decreased NAA and increased myoinositol. Pituitary adenomas can show only a choline peak; in the case of hemorrhagic complications, no metabolites are found.
1.4 Radiological Anatomy
1.4.1 The Anterior Lobe of the Pituitary Gland
In adults, the upper pole of the anterior lobe can be plane, concave, or convex. The signal of the normal anterior lobe is homogeneous, similar to that of the white matter of the temporal lobe on T1WI. A possible discrepancy between the size of the sella turcica and that of the pituitary gland can lead to mistakes. When the sella turcica is unusually small, the pituitary gland may appear bulky, overflowing frankly the theoretical plan of the sellar diaphragm in the manner of a brioche leaving its mold.
The size and morphology of the anterior lobe of the pituitary gland are variable according to age and sex (Fig. ).
Fig. 1.4
Pituitary gland in children, sagittal T1WIs. ( a ) 5-day-old newborn. Round and globulous pituitary gland. Anterior pituitary is markedly hyperintense and indistinguishable from the posterior lobe. ( b ) 12-day-old newborn. The convex anterior pituitary is hyperintense but slightly less so than the posterior pituitary. ( c ) 7-week-old infant. Convex upper pole of the pituitary gland. Hyperintensity of the anterior pituitary is less marked than that of the posterior pituitary. ( d ) 21-month-old child. The anterior pituitary gland is no more hyperintense. The posterior lobe is proportionally larger than in adult. ( e ) 7-year-old boy. No change when compared with ( d ). ( f ) 15-year-old girl. Normal convex pituitary gland of the adolescent