BarCharts - Nursing: Assessment
Here you can read online BarCharts - Nursing: Assessment full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2018, publisher: BarCharts, Inc., genre: Home and family. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
- Book:Nursing: Assessment
- Author:
- Publisher:BarCharts, Inc.
- Genre:
- Year:2018
- Rating:3 / 5
- Favourites:Add to favourites
- Your mark:
Nursing: Assessment: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Nursing: Assessment" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
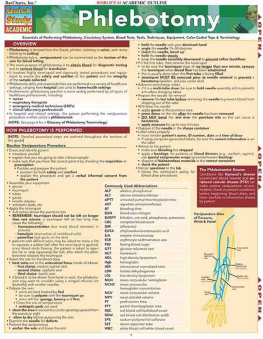
Our 3-panel (6-page) guidejam-packed with informationprovides a detailed review of a key aspect of the nursing profession: assessment. A perfect resource for nursing students or those already in the field who want to brush up on their skills, this guide covers the key concepts, skills and techniques essential to effective nursing assessment. Each section features The Nurse Knows summary of critical points, set off graphically for easy reference. Tables and images further enhance the text.
BarCharts: author's other books
Who wrote Nursing: Assessment? Find out the surname, the name of the author of the book and a list of all author's works by series.






Nursing: Assessment — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Nursing: Assessment" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:

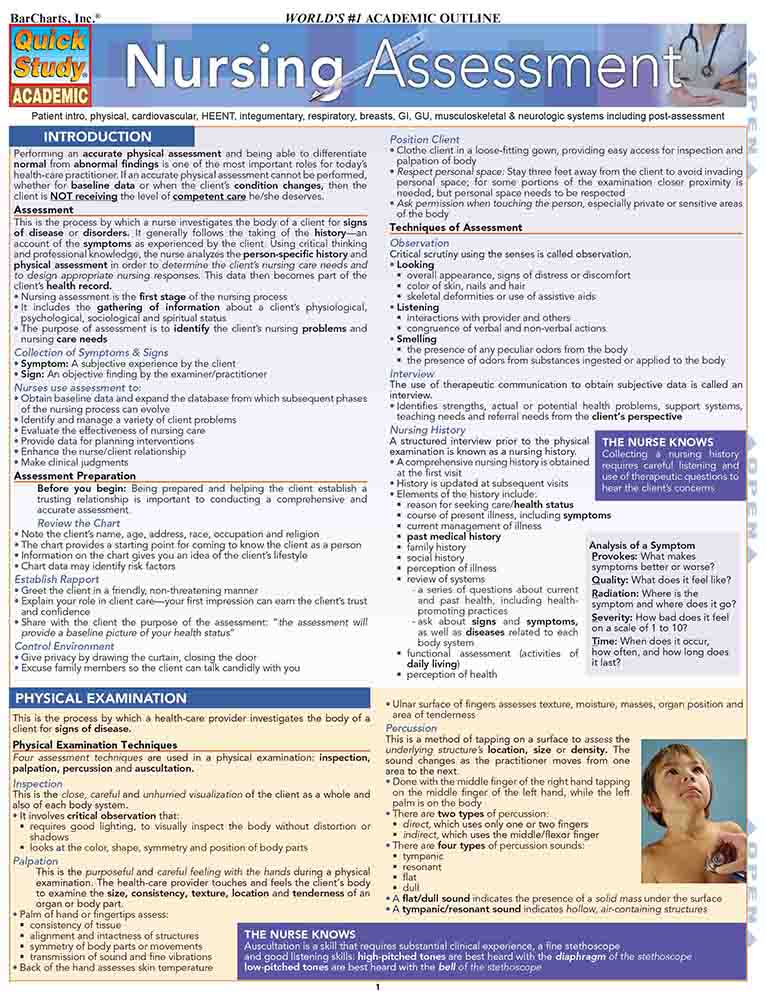
Patient intro, physical, cardiovascular, HEENT, integumentary, respiratory, breasts, GI, GU, musculoskeletal & neurologic systems including post-assessment
Performing an accurate physical assessment and being able to differentiatenormal from abnormal findings is one of the most important roles for todayshealth-care practitioner. If an accurate physical assessment cannot be performed,whether for baseline data or when the clients condition changes, then the client is NOT receiving the level of competent care he/she deserves.
AssessmentThis is the process by which a nurse investigates the body of a client for signsof disease or disorders. It generally follows the taking of the history an account of the symptoms as experienced by the client. Using critical thinkingand professional knowledge, the nurse analyzes the person-specific history andphysical assessment in order to determine the clients nursing care needs andto design appropriate nursing responses. This data then becomes part of theclients health record.
- Nursing assessment is the first stage of the nursing process
- It includes the gathering of information about a clients physiological,psychological, sociological and spiritual status
- The purpose of assessment is to identify the clients nursing problems and nursing care needs
- Symptom: A subjective experience by the client
- Sign: An objective finding by the examiner/practitioner
- Obtain baseline data and expand the database from which subsequent phasesof the nursing process can evolve
- Identify and manage a variety of client problems
- Evaluate the effectiveness of nursing care
- Provide data for planning interventions
- Enhance the nurse/client relationship
- Make clinical judgments
- Note the clients name, age, address, race, occupation and religion
- The chart provides a starting point for coming to know the client as a person
- Information on the chart gives you an idea of the clients lifestyle
- Chart data may identify risk factors
- Greet the client in a friendly, non-threatening manner
- Explain your role in client careyour first impression can earn the clients trustand confidence
- Share with the client the purpose of the assessment: the assessment willprovide a baseline picture of your health status
- Give privacy by drawing the curtain, closing the door
- Excuse family members so the client can talk candidly with you
- Clothe client in a loose-fitting gown, providing easy access for inspection andpalpation of body
- Respect personal space: Stay three feet away from the client to avoid invadingpersonal space; for some portions of the examination closer proximity isneeded, but personal space needs to be respected
- Ask permission when touching the person, especially private or sensitive areasof the body
- Looking
- overall appearance, signs of distress or discomfort
- color of skin, nails and hair
- skeletal deformities or use of assistive aids
- Listening
- interactions with provider and others
- congruence of verbal and non-verbal actions
- Smelling
- the presence of any peculiar odors from the body
- the presence of odors from substances ingested or applied to the body
The use of therapeutic communication to obtain subjective data is called aninterview.
- Identifies strengths, actual or potential health problems, support systems,teaching needs and referral needs from the clients perspective
Collecting a nursing historyrequires careful listening anduse of therapeutic questions tohear the clients concerns
A structured interview prior to the physicalexamination is known as a nursing history.
- A comprehensive nursing history is obtainedat the first visit
- History is updated at subsequent visits
- Elements of the history include:
- reason for seeking care/health status
- course of present illness, including symptoms
- current management of illness
- past medical history
- family history
- social history
- perception of illness
- review of systems
- a series of questions about currentand past health, including healthpromotingpractices
- ask about signs and symptoms,as well as diseases related to eachbody system
- functional assessment (activities ofdaily living)
- perception of health
Analysis of a Symptom
P rovokes: What makessymptoms better or worse?
Q uality: What does it feel like?
R adiation: Where is thesymptom and where does it go?
S everity: How bad does it feelon a scale of 1 to 10?
T ime: When does it occur,how often, and how long doesit last?
Four assessment techniques are used in a physical examination: inspection,palpation, percussion and auscultation.
InspectionThis is the close, careful and unhurried visualization of the client as a whole andalso of each body system.
- It involves critical observation that:
- requires good lighting, to visually inspect the body without distortion orshadows
- looks at the color, shape, symmetry and position of body parts
This is the purposeful and careful feeling with the hands during a physicalexamination. The health-care provider touches and feels the clients bodyto examine the size, consistency, texture, location and tenderness of anorgan or body part.
- Palm of hand or fingertips assess:
- consistency of tissue
- alignment and intactness of structures
Font size:
Interval:
Bookmark:
Similar books «Nursing: Assessment»
Look at similar books to Nursing: Assessment. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Nursing: Assessment and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.