David Alberts and Lisa M. Hess (eds.) Fundamentals of Cancer Prevention 3rd ed. 2014 10.1007/978-3-642-38983-2_1
Springer-Verlag Berlin Heidelberg 2014
1. Introduction to Cancer Prevention
Abstract
The goals of cancer prevention are to reduce the incidence, morbidity, and mortality due to cancer through the identification and elimination of precancerous lesions (termed intraepithelial neoplasias or IENs) and/or the early detection of minimally invasive cancers. Between 2001 and 2009, the USA saw an average 1.6 % annual reduction in the total number of cancer deaths (Howlader et al., 2012). While declining death rates have been seen for all racial and ethnic groups in the USA, there have been smaller reductions among women than men and smaller reductions in deaths among African Americans as compared to populations with a European heritage (Jemal et al., 2010). These reductions were primarily due to advances in and improved access to cancer detection and prevention efforts, resulting in less exposure to risk factors such as tobacco (Jemal et al., 2010). As a result, an estimated 767,100 cancer deaths have been averted over the past two decades in the USA (Jemal et al., 2010). These averted deaths are largely driven by reductions in lung cancer (reduction in tobacco use), stomach cancer (reduced H. pylori infections and improved food storage and preservation methods), breast cancer and colorectal cancer (due to improved screening and treatment modalities), cervical cancer (Pap testing and the HPV vaccine), as well as lymphoma, leukemia, and testicular cancer (due to new treatments). Unfortunately, other cancers have increased, such as liver cancer (increasing hepatitis C infections), esophageal cancer (associated with increasing obesity and gastric reflux disease), pancreatic cancer, and melanoma (due to sun exposure). Despite the recent reduction in incidence and mortality rates, cancer remains the second leading cause of mortality in the USA (responsible for over 580,000 deaths per year) (Siegel et al., 2013). For Americans from the age of 4079, cancer is the leading cause of death (Siegel et al., 2013). Only at age 80 and older does heart disease surpass cancer. Therefore, it is extremely important that we continue to prioritize efforts in cancer prevention and control to reduce the impact of these diseases.
1.1 Introduction
The concept of cancer prevention is changing gradually as we gain a greater understanding of the genetic and molecular basis of carcinogenesis. Certainly, it is understood that the cancer patient is not well one day and the next day diagnosed with cancer. It is estimated that there is an average lag of at least 20 years between the development of the first cancer cell and the onset of end-stage metastatic disease for a broad range of solid tumors. In that there were an estimated 1,660,290 new cancer cases and 580,350 cancer deaths in the USA in 2013 (Siegel et al. ) and given the 20+-year lag time, more than 11 million healthy Americans currently harbor ultimately deadly cancers, many of which may be fully preventable.
Given the average 20-year lag time from the point of the first altered cell to carcinoma, secondary and tertiary prevention strategies represent effective and cost-effective opportunities to dramatically reduce cancer mortality in the next decades. Cancer costs exceeded US$201.5 billion in 2008 alone (ACS discusses the human and economic benefits of cancer prevention in more detail.
1.2 Summary of Changes to Third Edition
In 2009, the Union of International Cancer Control Annual Report stated that our current knowledge shows that 40 % of cancers can be prevented and 2533 % can be avoided by eating a healthy diet, maintaining a healthy body weight, and remaining physically active; however, the tragedy is that we are not using this knowledge to reduce the global burden of cancer (UICC ). The dissemination of complicated information is problematic, but comprehensive information is essential to reduce the burden of cancer. The third edition of this book is designed to provide this information in the form of a comprehensive overview on the science and practice of cancer prevention for primary caregivers and the research community.
Because of the rapid advancement in cancer prevention research, several important changes have been made to the third edition of this book. The first section of this book (, discussing issues related to cancer survivorship.
The field of cancer prevention is constantly changing as research progresses and our knowledge about cancer expands. Each chapter has been revised in the third edition. Important new chapters in this revised edition include ), which focuses on cancer as a global issue that our world is facing.
1.3 Overview of Cancer Prevention
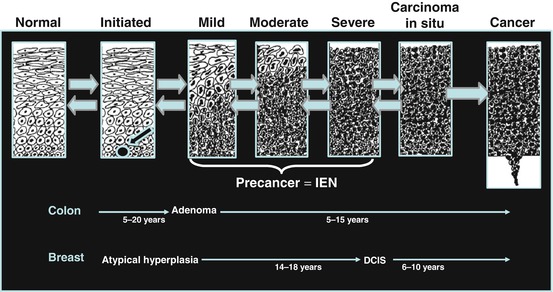
Cancer is a global term for a variety of diseases that share some similar characteristics, such as uncontrolled cellular growth, enhanced angiogenesis, and/or reduced programmed cell death. The site of origin of the disease is used to define general categories of disease (e.g., breast cancer, skin cancer). It is increasingly apparent that despite the variation across cancer types, the majority of cancers proceed from the first initiated tumor cell (e.g., mutated DNA) to mild, moderate, and severe dysplasia, invasive carcinoma (invasion of cells through the basement membrane), and metastatic disease (Fig. ). They are represented by small, intermediate, and advanced adenomatous polyps in the colon; atypical hyperplasia and ductal carcinoma in situ in the breast; and simple hyperplasia, atypical hyperplasia, and carcinoma in situ in the endometrium. As atypia increases, these dysplasias are believed to develop into cancer and if left unchecked have the great potential to metastasize to adjacent and distant organs.
Fig. 1.1
Progression of precancer to cancer in humans is a multiyear process (Adapted from OShaughnessy et al. ())
It is estimated that there are over 12.7 million cases of cancer diagnosed and 7.6 million deaths each year worldwide (Jemal et al. ). The highest rates of esophageal cancer are found in Eastern Asia and East Africa, and half of all liver cancers are diagnosed in China.
Table 1.1
Worldwideannual cancer incidenceand mortality of selected common cancers(Jemal et al. )
| Number of new cases each year | Number of deathseach year |
|---|
Males |
Lung | 1,095,200 | 951,000 |
Prostate | 903,500 | 258,400 |
Colon/rectum | 663,600 | 320,600 |
Stomach | 640,600 | 464,400 |
Liver | 522,400 | 478,300 |
Esophagus | 326,600 | |