Reich - Selling our souls : the commodification of hospital care in the United States
Here you can read online Reich - Selling our souls : the commodification of hospital care in the United States full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. City: Princeton, year: 2014, publisher: Princeton University Press, genre: Romance novel. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
- Book:Selling our souls : the commodification of hospital care in the United States
- Author:
- Publisher:Princeton University Press
- Genre:
- Year:2014
- City:Princeton
- Rating:4 / 5
- Favourites:Add to favourites
- Your mark:
Selling our souls : the commodification of hospital care in the United States: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Selling our souls : the commodification of hospital care in the United States" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Health care costs make up nearly a fifth of U.S. gross domestic product, but health care is a peculiar thing to buy and sell. Both a scarce resource and a basic need, it involves physical and emotional vulnerability and at the same time it operates as big business. Patients have little choice but to trust those who provide them care, but even those providers confront a great deal of medical uncertainty about the services they offer. Selling Our Souls looks at the contradictions inherent in one particular health care market--hospital care. Based on extensive interviews and observations across the three hospitals of one California city, the book explores the tensions embedded in the market for hospital care, how different hospitals manage these tensions, the historical trajectories driving disparities in contemporary hospital practice, and the perils and possibilities of various models of care.
As Adam Reich shows, the books three featured hospitals could not be more different in background or contemporary practice. PubliCare was founded in the late nineteenth century as an almshouse in order to address the needs of the destitute. HolyCare was founded by an order of nuns in the mid-twentieth century, offering spiritual comfort to the paying patient. And GroupCare was founded in the late twentieth century to rationalize and economize care for middle-class patients and their employers. Reich explains how these legacies play out today in terms of the hospitals different responses to similar market pressures, and the varieties of care that result.
Selling Our Souls is an in-depth investigation into how hospital organizations and the people who work in them make sense of and respond to the modern health care market.
Reich: author's other books
Who wrote Selling our souls : the commodification of hospital care in the United States? Find out the surname, the name of the author of the book and a list of all author's works by series.



Selling our souls : the commodification of hospital care in the United States — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Selling our souls : the commodification of hospital care in the United States" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Selling Our Souls
Selling Our Souls
THE COMMODIFICATION OF HOSPITAL CARE IN THE UNITED STATES
Adam D. Reich
Princeton University Press
Princeton and Oxford
Copyright 2014 by Princeton University Press
Published by Princeton University Press, 41 William Street, Princeton, New Jersey 08540
In the United Kingdom: Princeton University Press, 6 Oxford Street, Woodstock, Oxfordshire OX20 1TW
press.princeton.edu
Jacket art intune123/123RF
All Rights Reserved
Library of Congress Cataloging-in-Publication Data
Reich, Adam D. (Adam Dalton), 1981
Selling our souls : the commodification of hospital care in the United States / Adam D. Reich.
pages cm
Includes bibliographical references and index.
ISBN 978-0-691-16040-5 (hardcover)
1. Hospital care. 2. HospitalsBusiness management. 3. Hospital careCost effectiveness.
I. Title.
RA971.3.R35 2014
362.11dc23
2013034451
British Library Cataloging-in-Publication Data is available
This book has been composed in Minion Pro
Printed on acid-free paper.
Printed in the United States of America
10 9 8 7 6 5 4 3 2 1
For Ella
Contents
Selling Our Souls
Introduction
The hospital has a paradoxical place in U.S. society. Such contradictions, between the mission of hospital care and the market for it, are the focus of this book.
The United States is unique among modern industrial nations in the extent to which it has relied on the market to determine the organization and allocation of hospital (and all health care) services. By market I mean, most basically, the principle of exchange for profit or gain. The market has played an important role in the organization of the American hospital since at least the first decades of the twentieth century. Still, over the past forty years, public health concerns, professional autonomy, and charitable impulses have given way even more dramatically to a focus on profit making and the bottom line.
Since all hospitals today must compete for the dollars that accompany patient utilization, all are under pressure to engage in similar practices, such as reducing the amount of free care they provide, investing heavily in capital improvements,
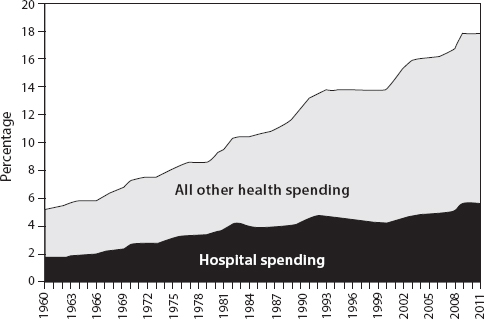
I.1. Health expenditures as percentage of GDP, 19602011.
Centers for Medicare & Medicaid Services, 2012.
Health spending has continued a seemingly inexorable increase as a proportion of gross domestic product, reaching nearly 18 percent in 2010. This rise can be seen both as a cause and a consequence of the ascendance of market actors and market logics across the health care industry.
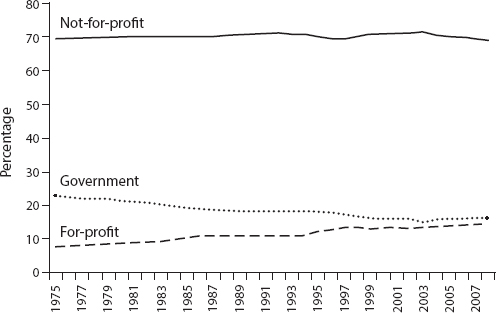
I.2. Percentage of short-term hospital beds by type of control, 19752008.
American Hospital Association, Hospital Statistics.
Market actors wield tremendous power within the hospital industry, but they are not the entire story. Despite market pressures, between 1975 and 2008 the percentage of hospital beds under the control of not-for-profit organizations remained virtually unchanged at around 70 percent (see
Moreover, the development of the hospital market has been mitigated historically by a variety of institutional rules and norms that buffer hospital care from the markets worst excesses. The recently passed Patient Protection and Affordable Care Act, or Obamacare, intervenes in the market along these lines, changing the broader rules of the game byfor exampleincreasing access to health insurance for the currently uninsured and incentivizing evidence-based medical practice and quality outcomes. (For more about this legislation, see Conclusion in this book.)
So while market forces and market actors have become increasingly important to contemporary hospital practice, the commodification of hospital care in At the same time that hospitals compete in a competitive marketplace, many hospitalsand the people within themwork to sustain social values that sit in uneasy tension with this market.
Welcome to Las Lomas
In order to understand these contradictions, we must look not only at the broad sets of rules and regulations through which the market for hospital care is structured but also at the meanings, practices, and people that make up the hospital itself. This book is a detailed study of three hospitals within the same medium-sized city of Las Lomas. Each hospital was founded in a different era of American medicine to serve a different kind of patient and solve a different sort of problem. Today, these historical legacies frame each hospitals ongoing struggle with a different contradiction in the commodification of hospital care, as each worksimperfectlyto reconcile the social values on which it was founded with the imperatives of the competitive marketplace. (For a detailed discussion of methods, see A Note on Methods in this book.)
Located within a few miles of one another, PubliCare, HolyCare, and GroupCare serve as the only major hospital facilities in the larger 500,000-person county. Each is a part of a different not-for-profit health system (PubliCare previously had been the countys public hospital but was privatized in 1996). Each considers the other two as its primary competitors for the countys pool of insured patients. The three hospitals offer many of the same services, and they face many of the same market pressures. Despite these similarities, however, they are in many ways worlds apart.
Katherine Taylor, a nurse manager at GroupCare, had strong opinions about all three. We spoke together while sitting on flimsy plastic chairs on a small patio just outside GroupCares basement cafeteria. Taylor remembered getting into the nursing profession because of a desire to care for people in difficult times. She had a particular affinity for children, she said, and assumed she would become a pediatric nurse. But this same emotional connection she felt with kids ultimately made pediatrics overwhelming: Because I love them so much [it] was really hard for me, to deal with my emotions around it. And solike many other nurses I would come to meet in the cityTaylor had found ways to manage her emotional vulnerability at work. She realized that she either would have to shut down or would have to find another area of hospital practice. Taylor found the intensive care unit: I have a very fast-working brain, so it was just the constant stimulation: information, machines, critical patients. It kept me on the edge of my seat for the whole twelve hours I was working. So that was really enticing for me. She would escape her vulnerability in the pediatrics ward via the frenetic hum of critical care.
Taylor had been working in Las Lomas for the last fifteen years as a critical care nurse and nurse manager. During this time she had been employed at each of the three hospitals. PubliCare, she thought, was remarkable for the mutual respect among the doctors and the nursing staff there: It was a rare moment at PubliCare that we would have a physician be rude, obnoxious, disrespectfulany of that. But this egalitarianism, she thought, sometimes digressed into a kind of sloppiness: The nurses would sit at the nurses station and laugh at the physicians, talk about things that I was, like, Oh! Ugh! What?! People dressed a little flowerier and funkier than she was used to. And while the care was pretty good, she did not think it was exceptional. No one seemed particularly concerned with national hospital standards: Compliance wasnt really part of what they talked about at PubliCare. Taylor worked her way into a more managerial role at PubliCare and helped oversee an inspection during which the hospital almost lost its accreditation. But she liked the place and loved the people: The people are delightful. Physicians were delightful. It had this great personality, but it really needed to rise up to the level of, you know, clean, competent. The manager before she arrived was a real hippie.
Next pageFont size:
Interval:
Bookmark:
Similar books «Selling our souls : the commodification of hospital care in the United States»
Look at similar books to Selling our souls : the commodification of hospital care in the United States. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Selling our souls : the commodification of hospital care in the United States and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.