Douglas R. Lazzaro - Diabetes and the Eye: Latest Concepts and Practices
Here you can read online Douglas R. Lazzaro - Diabetes and the Eye: Latest Concepts and Practices full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. City: Singapore, year: 2021, publisher: Bentham Science Publishers, genre: Science. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
- Book:Diabetes and the Eye: Latest Concepts and Practices
- Author:
- Publisher:Bentham Science Publishers
- Genre:
- Year:2021
- City:Singapore
- Rating:5 / 5
- Favourites:Add to favourites
- Your mark:
Diabetes and the Eye: Latest Concepts and Practices: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Diabetes and the Eye: Latest Concepts and Practices" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Douglas R. Lazzaro: author's other books
Who wrote Diabetes and the Eye: Latest Concepts and Practices? Find out the surname, the name of the author of the book and a list of all author's works by series.



Diabetes and the Eye: Latest Concepts and Practices — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Diabetes and the Eye: Latest Concepts and Practices" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Andrew M. Hendrick
The incidence of diabetes mellitus is increasing worldwide. Over time, diabetes is associated with the development of diabetic retinopathy, a major cause of vision loss globally. Research has demonstrated factors associated with the onset and progression of the disease. Despite advancements in understanding the importance of optimizing care, the cases of vision loss due to diabetic retinopathy are also increasing. The epidemic of this systemic disease and the retinal manifestations will be discussed in detail in this chapter.
Diabetes mellitus (DM) is a chronic health condition defined by the presence of impaired glucose regulation leading to hyperglycemia. Normal blood sugar levels depend on the effective use of insulin, a peptide hormone responsible for triggering glucose uptake into cellular spaces (among many other critical metabolic effects). In people with diabetes mellitus, insulin is not used effectively; this is either due to underproduction as seen in type 1 diabetes mellitus (T1DM), or end-tissue resistance to the effects of insulin as seen in type 2 diabetes mellitus (T2DM). Longstanding and/or poorly controlled elevated blood sugar levels are major determinants of complications from DM such as cardiovascular disease, nerve damage, renal disease, and eye disease including retinopathy [].
The two major subdivisions of diabetes mellitus have several distinguishing characteristics. T1DM results from an auto-immune attack of the insulin-producing pancreatic islet cells, typically during childhood. The onset of T1DM can be dramatic with diabetic ketoacidosis but can be more insidious, characterized by poor growth. T1DM requires insulin injections as the fulcrum of
therapy to normalize blood sugar levels and are required for survival. In contrast, T2DM results from dysfunction of insulin response, such that circulating glucose levels remain elevated [].
Our world is in the midst of a diabetes mellitus epidemic with rising rates of people affected across the globe. Factors driving the increase include population aging, economic development, increased urbanization, sedentary lifestyle, and increased consumption of unhealthy foods []. The risk of developing complications is tied directly to the adequacy of medical management. Managing the disease and associated health-related consequences, such as blinding complications of retinopathy, is becoming increasingly important as all societies struggle with this burden. This chapter will discuss the epidemiology of diabetes mellitus, with a focus on diabetic retinopathy (DR) and the implications for vision loss.
T1DM accounts for nearly 10% of DM cases and the incidence has slightly increased over time, with considerable variation by region and sampling technique [].
90% of all people with DM have T2DM, also known as adult-onset diabetes. As a result, global estimates of diabetes are predominantly reflective of change due to T2DM. T2DM is increasingly more common - likely due to the strong association with obesity, population aging, inactive lifestyle and poor dietary habits [].
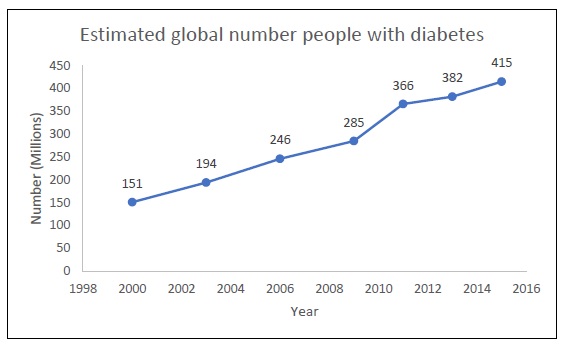
Estimated number of people with diabetes over time worldwide (in millions) [].
The fallout from chronic hyperglycemia on the human body is accumulative over time. Morbidity and disability that arises from serious complications of diabetes include cardiovascular disease, kidney disease, neuropathy, limb amputation, and retinopathy. These complications, in turn, lead to an increased demand for medical care, reduce the quality of life, and place stress on families including financial burden. Altogether, diabetes-related care incurs an estimated $673 billion (12%) of global healthcare expenditure and 8% of all-cause mortality [].
Ocular complications of diabetes include a spectrum of pathologies that range from refractive error and increased risk of cataract formation to cranial nerve palsies and blindness from diabetic retinopathy (DR) [].
Earliest estimates on the epidemiology of DR came from the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR). The WESDR was a population-based study conducted on a predominantly Caucasian cohort with both T1DM and T2DM in the 1980s. In this study, which has now accrued decades of follow up, it became possible to understand the increased risk of diabetic retinopathy progression over time [].
At the time of WESDR, it was not yet established that euglycemia was critical for risk factor modification in preventing retinopathy progression [].
The prevalence of DR is widely varied due to variations in timing and characteristics of the snapshot of the defined population [].
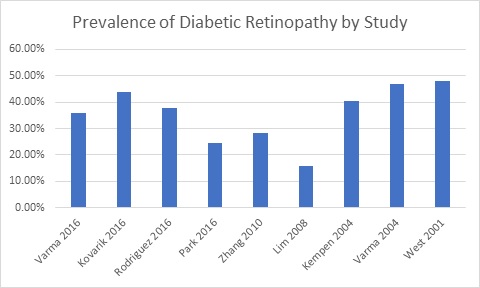
The prevalence of diabetic retinopathy varies depending on the population characteristics and sampling techniques employed [].
The epidemiology of DME is of great interest due to its impact on quality of vision, but difficult to compare due to variations in definition of the disease. Studies vary with use of clinical examination, fundus photography and optical coherence tomography based definitions [].
Racial and ethnic impact on the epidemiology of DR is of great interest because of the wide differences in the reported rates of DR prevalence and the implications for environmental versus genetic influence. From the US, the third National Health and Nutrition Examination Survey (NHANES III) was a cross sectional study from the Center for Disease Control and Prevention from 1988-1994 to determine if racial and or ethnic differences modulated the risk of developing DR. This study demonstrated that Mexican-American participants had higher rates of DR compared to non-Hispanic white participants (33.4% vs 18.2%) [].
Genetics also contribute to susceptibility of DR onset and severity. Analysis of the Diabetes Control and Complications Trial (DCCT) indicates that glycemic control, as was reflected by hemoglobin A1c levels, was beneficial in reducing the incidence of DR [], The overall importance of genetics in determinants of diabetes related complications is an ongoing area of investigation.
Due to the asymptomatic nature of DR, individuals with diabetes should be properly screened for signs of DR and the progressive stages of DR. At a minimum, screening guidelines suggest a dilated fundus examination on an annual basis for T2DM and T1DM, beginning 5 years after diagnosis [].
Studies suggest that there is poor adherence to recommended guidelines such that an estimated nearly half of people with diabetes do not routinely receive an eye exam [].
Overall, type 1 diabetes represents a minority of cases of diabetes mellitus with indications that the disease is becoming slightly more common over time. Although people with T1DM have higher rates of ocular complications than people with T2DM, incident retinopathy has reduced with improved control of systemic management. In contrast, type 2 diabetes is much more prevalent, and the prevalence is increasing over time worldwide with substantial regional variation. Similar increasing trends are noted when examining the epidemiology of diabetic retinopathy.
Font size:
Interval:
Bookmark:
Similar books «Diabetes and the Eye: Latest Concepts and Practices»
Look at similar books to Diabetes and the Eye: Latest Concepts and Practices. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Diabetes and the Eye: Latest Concepts and Practices and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.