Michael H. Weisman - Ankylosing Spondylitis
Here you can read online Michael H. Weisman - Ankylosing Spondylitis full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2011, publisher: Oxford University Press, USA, genre: Home and family. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Ankylosing Spondylitis
- Author:
- Publisher:Oxford University Press, USA
- Genre:
- Year:2011
- Rating:4 / 5
- Favourites:Add to favourites
- Your mark:
Ankylosing Spondylitis: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Ankylosing Spondylitis" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Michael H. Weisman: author's other books
Who wrote Ankylosing Spondylitis? Find out the surname, the name of the author of the book and a list of all author's works by series.

Ankylosing Spondylitis — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Ankylosing Spondylitis" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
MICHAEL H. WEISMAN, MD

Oxford University Press, Inc., publishes works that further Oxford University's
objective of excellence in research, scholarship, and education.
Oxford New York
Auckland Cape Town Dar es Salaam Hong Kong Karachi
Kuala Lumpur Madrid Melbourne Mexico City Nairobi
New Delhi Shanghai Taipei Toronto
With offices in
Argentina Austria Brazil Chile Czech Republic France Greece
Guatemala Hungary Italy Japan Poland Portugal Singapore
South Korea Switzerland Thailand Turkey Ukraine Vietnam
Copyright 2011 by Oxford University Press, Inc.
Published by Oxford University Press, Inc.
198 Madison Avenue, New York, New York 10016
www.oup.com
Oxford is a registered trademark of Oxford University Press
All rights reserved. No part of this publication may be reproduced, stored in a
retrieval system, or transmitted, in any form or by any means, electronic, mechanical,
photocopying, recording, or otherwise, without the prior permission
of Oxford University Press.
Library of Congress Cataloging-in-Publication Data
Weisman, Michael H.
Ankylosing spondylitis / Michael H. Weisman. p. ; cm.
Includes bibliographical references and index. ISBN 978-0-19-539910-3
1. Ankylosing spondylitisPopular works. I. Title.
[DNLM: 1. Spondylitis, AnkylosingPopular Works. WE 725]
RD771.A5W45 2011
616.7'3dc22 2010041913
9 8 7 6 5 4 3 2 1
Printed in USA
on acid-free paper
CONTENTS
PART TWO WHERE AND HOW THE
BODY CAN BE AFFECTED BY
ANKYLOSING SPONDYLITIS
AND OVERVIEW
THE FIRST CHAPTER in this section,
Spondylitis
ANKYLOSING SPONDYLITIS (AS) is one of several conditions that belong to a group of chronic inflammatory rheumatic disorders known as spondyloarthropathies (SPAs). It is a chronic systemic inflammatory disease that primarily attacks the axial skeleton and adjacent structures. The axial skeleton () consists of 80 bones in the head and trunk of the body, and is divided into five parts: skull, ossicles of the inner ear, hyoid bone of the throat, rib cage, and the vertebral column.
Typically, the vertebrae of the spine become inflamed, causing chronic pain and discomfort. In more severe cases, this inflammation can lead to new bone formation on the spine, causing the spine to fuse in a fixed, immobile position resulting in a forward-stooped posture. If left untreated, the inflammation of the spinal joints will gradually destroy the cartilage and fibrous tissue of the surrounding structures as well as the ligaments and literally replace them with bone. There appears to be a cyclical process to the disease (). Interrupting this cycle with early identification of the disease and aggressive treatment may prevent the immobility and stooped posture caused by spinal fusion.
The effects of AS are not confined to the spine. Patients with AS may experience pain and inflammation in other joints, such as hips, shoulders, knees, elbows, and feet. Ankylosing spondylitis may also affect the lungs, eyes, bowel and, in rare cases, the heart. There is a considerable genetic and clinical overlap between AS and inflammatory bowel disease, the causes of which are being investigated. Details of the effects of AS on other parts of the body, and the signs, symptoms, and treatment of conditions associated with AS will be discussed in later chapters.
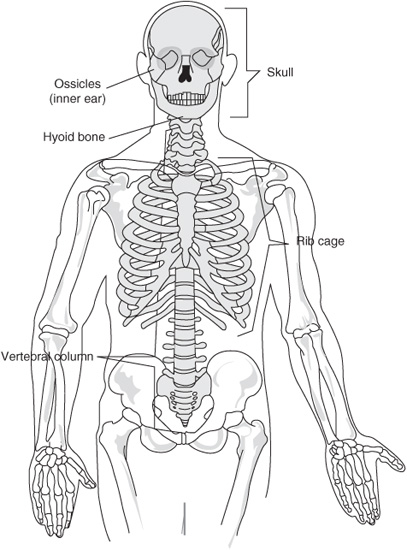
FIGURE 1.1 Axial Spine
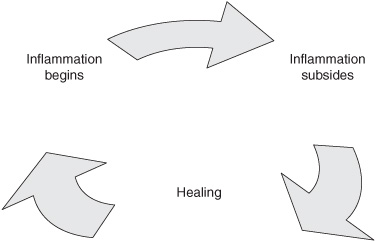
FIGURE 1.2 AS Inflammatory Disease Process
The diagnosis of AS is based on clinical features and radiographic (X-ray) criteria. Unfortunately, there are no laboratory tests that can be used to establish a diagnosis of AS with certainty. The modified New York 1984 criteria () are the most commonly used criteria to classify AS. Diagnostic criteria for AS have been recommended, but have not been validated through scientific study.
Classification criteria for AS, and other rheumatic diseases such as rheumatoid arthritis, are used to identify patients for research and genetic studies. To be useful for research, treatment protocols, and genetic studies, it is important that the classification criteria correctly and definitively identify patients with the disease. This means that the usual classification criteria identify patients with a disease that is recognizable and quite certainly established with little doubt. Because classification criteria almost always require changes in the body that indicate that the disease has been present for some time, it is difficult to develop diagnostic criteria ahead of permanent damage. In the case of AS, classification criteria require X-ray evidence of damage to the spine. However, we want to diagnose AS patients before spinal damage has occurred; therefore, any diagnostic criteria need to be based on a probability that the patient has AS. This is the challenge that physicians face today in diagnosing ASto develop diagnostic criteria that we can apply earlier in the course of disease and before damage has occurred to the spine. In other words, we want to diagnose patients with AS before or ahead of the time they fulfill classification criteria.
Table 1.1
MODIFIED NEW YORK CLASSIFICATION CRITERIA
FOR ANKYLOSING SPONDYLITIS
Clinical Components |
Low back pain and stiffness for 3 months that improves with exercise but not with rest |
Limitation of lumbar spine mobility in both the sagittal (sideways) and frontal (forward and back) planes |
Limitation in chest expansion as compared with normal range for age and gender |
Radiologic Component |
Unilateral sacroiliitis of Grade 3 or 4, or bilateral sacroiliitis of Grade 2 |
Diagnosis |
Definite AS if the radiological criterion is associated with at least one clinical component |
Probable AS if: |
Only the three clinical components are present or |
Only the radiologic component is present |
Fortunately, new classification criteria recently developed and refined by the Assessment of SpondyloArthritis international Society (ASAS) provide guidelines to aid in the diagnosis of patients prior to the appearance of positive radiographic findings.
Spondylitis
THE WORDS ankylosing and spondylitis are of Greek origin. Angylos means bent or crooked, and refers to the stooped or bent posture that may occur in AS patients. Spondylos means spinal vertebrae, and itis means inflammation. Spondylitis, then, is an inflammation of the vertebrae. The historical dating of ankylosing spondylitis (AS) is controversial and remains the subject of considerable debate, with some investigators dating the first incidence of AS to antiquity, while others contend that AS is of more recent origin. Based on paleopathologic studiesthe study of diseases in ancient remains or medical writingsa number of researchers have concluded that evidence from humans and animals indicates that the origins of AS go as far back as several thousand years BC. For example, Egyptian pharaohs, including Amenhotep II (reign 14271401 BC), Ramses the Great (reign 12791213 BC), and Ramses son Merneptah (reign 12131203 BC), have been described as having AS. During the fifth century, Hippocrates, author of the Hippocratic oath by which all physicians are bound to ethically practice medicine, described a condition suggestive of AS. Other researchers have determined that ancient cases of AS are more likely cases of a condition known as
Font size:
Interval:
Bookmark:
Similar books «Ankylosing Spondylitis»
Look at similar books to Ankylosing Spondylitis. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Ankylosing Spondylitis and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.