Neil S. Sadick , Neil Khilnani and Nick Morrison (eds.) Practical Approach to the Management and Treatment of Venous Disorders 2013 10.1007/978-1-4471-2891-5_1 Springer-Verlag London 2013
1. Phlebology: History and Epidemiology
Abstract
It may be that anatomic research on the veins, and especially on the valves in the veins, is responsible for all of the advances of the Twentieth Century in Cardiovascular Medicine and surgery. It is agreed that the studies and subsequent illustrations of the venous valves by Fabricius led Harvey to create his mental conception of the circulation. Before that, the Ebers Papyrus had described certain serpentine windings, which, were not to be operated upon lest that lead to head on the ground. Clearly, experience had taught that incision into varicosities could be fatal.
In the case of an ulcer, it is not expedient to stand; more especially if the ulcer be situated in the leg. []
Hippocrates (460377 BC)
It may be that anatomic research on the veins, and especially on the valves in the veins, is responsible for all of the advances of the Twentieth Century in Cardiovascular Medicine and surgery. It is agreed that the studies and subsequent illustrations of the venous valves by Fabricius led Harvey to create his mental conception of the circulation. Before that, the Ebers Papyrus had described certain serpentine windings, which, were not to be operated upon lest that lead to head on the ground []. Clearly, experience had taught that incision into varicosities could be fatal.
Judging by the much-reproduced illustration (see Browse, NL Diseases of the Veins and Bergan, JJ Venous Disorders ) of the votive offering of Lysimachidis to Dr Amynous, the ancients were referring not to telangiectases but instead to gross varices. It was these that certainly should not be incised. One can only guess what treatment Dr Amynous employed to stimulate such a grand gift.
Curious Theories
Unproven opinions about the veins and their functioning dominated medical thought from the eleventh to the last half of the nineteenth century. These were obviously influenced by the black bile theory of Galen [].
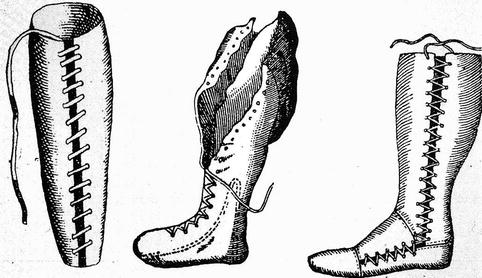
Richard Wiseman, Sergeant Surgeon to Charles II invented the leather lace up stocking for treatment of the symptoms of venous disease [).
Fig. 1.1
Compression therapy as delivered by Wisemans laced up leather stocking was and is effective in ameliorating symptomatic venous stasis
Fast forwarding to the sixteenth century, it is remarkable to find that Fabricius (15331620) not only named the valves in the veins in 1603 but also stated that they were placed to delay the blood from flooding into the feet or hands and fingers and collecting there [).
Fig. 1.2
Fabricius published his De venarum ostiolis in 1603 as an unbound folio pamphlet accompanied by eight engraved plates, which has been described as one of the most beautiful works in the history of anatomy
The objectives of the modern surgical treatment of varicose veins were described by a number of surgeons at the end of the nineteenth century. Madelung in 1880s excised the Saphenous vein through a groin to knee incision that entailed considerable morbidity and, in those days, prolonged hospitalization [].
It is my opinion, not shared by many that the importance of the role of incompetent calf perforators and other perforating veins as stressed in many instructions on performance of varicose vein surgery and as advocated by Cockett and many others represents a step backward on acceptance of evidence based medicine in Phlebology []. Evidence based medicine as introduced by Trendelenburg more than 100 years ago has had a hard time in Phlebology.
Minimally Invasive Varicose Vein Treatment
In an attempt to minimize postoperative discomfort and yet maintain the benefits of Saphenous vein ablation, electromagnetic waves have been applied to affect rapid thermic electrocoagulation of the vein wall and its valves []. The energy is supplied as radio frequency (RF) and Laser energy (EVLT). Prolonged exposure to such energy results in total loss of vessel wall architecture, disintegration and carbonization.
The objective of applying electromagnetic energy to vein intima is to remove the refluxing Saphenous vein from the circulation in a manner that minimizes patient discomfort, decreases postoperative morbidity, provides a good long-term outcome and allows rapid return of the patient to normal activities []. Since elimination of the refluxing saphenous vein from the circulation is the only goal of the procedure, judgment of success can be assessed by duplex ultrasound at any time postoperatively. Relief of patient symptoms, time to resume normal activities, post-procedure adverse events, and improvement in health-related quality of life are additional relevant measures of the procedure outcome. However, these are linked to successful elimination of saphenous vein reflux.
Unlike Saphenous vein stripping, the RF and EVLT procedures do not require a general anesthetic and can be performed using local high volume or intracompartmental infiltration anesthesia with or without conscious sedation. These can usually be performed on an outpatient basis in a surgicenter or low cost settings such as a minor procedures room or an office setting.
Early and 5 year outcomes data and ultrasound scans clearly show that endovenous obliterations successfully remove refluxing Saphenous veins from the circulation in approximately 90% of treatments [].
Now there is Level I evidence which documents success of the technique. Furthermore, removal of the Saphenous vein from circulation has been carefully studied and reported in separate series. Pichot observed that serial duplex ultrasound scans showed the RF treated Saphenous veins to be progressively more echogenic and shrunken until they were incorporated into the surrounding tissue [].
Increasingly, some clinicians believe that endovenous obliteration is a better operation than vein stripping since endovenous treatment preserves abdominal wall drainage and this prevents neovascularization, the most common cause of recurrence after proper vein stripping surgery [].
Ascent of Foam Sclerotherapy
After 100 years of surgical therapy for varicose veins, a truly minimally invasive therapy has emerged. It started as early as 1939 and has continuously been improved up to the present time. Many lesser-known colleagues, such as Orbach and Flckiger, have made many contributions [].
Administration of foamed sclerosant was re-introduced in the early 1990s by Cabrera, who vsummarized a broad experience in 1997 []. Emphasis in the past 10 years of using foamed sclerosant has been confined for the most part to reports of treating varices and refluxing saphenous trunks but our experience in treating CVI is very encouraging.
In treating varicose veins, all published reports describe efficacy in terms of immediate and primary venous occlusion of better than 80% []. Repetition of injections in cases of initial failure allows the results to approach 95% efficacy with three sessions. Early and mid term results to >5 years demonstrate a recurrence rate of about 20%. Treating recurrences by injections is as simple as primary treatment and is at least as effective.