Reason - Organizational Accidents Revisited
Here you can read online Reason - Organizational Accidents Revisited full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. City: Brookfield, year: 2016, publisher: Taylor & Francis Ltd;CRC Press, genre: Romance novel. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Organizational Accidents Revisited
- Author:
- Publisher:Taylor & Francis Ltd;CRC Press
- Genre:
- Year:2016
- City:Brookfield
- Rating:5 / 5
- Favourites:Add to favourites
- Your mark:
Organizational Accidents Revisited: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Organizational Accidents Revisited" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Reason: author's other books
Who wrote Organizational Accidents Revisited? Find out the surname, the name of the author of the book and a list of all author's works by series.

Organizational Accidents Revisited — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Organizational Accidents Revisited" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
To Thomas Augustus Reason (18791958).
My grandfather to whom I owe much more than my existence.
JAMES REASON
Professor Emeritus, University of Manchester, UK
ASHGATE
First published 2015 by Ashgate Publishing
Published 2016 by Taylor & Francis
2 Park Square, Milton Park, Abingdon, Oxon OX14 4RN
711 Third Avenue, New York, NY 10017
Ashgate is an imprint of the Taylor & Francis Group, an informa business
James Reason 2016
All rights reserved. No part of this book may be reprinted or reproduced or utilised in any form or by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying and recording, or in any information storage or retrieval system, without permission in writing from the publishers.
James Reason has asserted his right under the Copyright, Designs and Patents Act, 1988, to be identified as the author of this work.
www.ashgate.com
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British Library
The Library of Congress has cataloged the printed edition as follows:
A catalogue record for this book is available from the Library of Congress
ISBN: 9781472447654 (hbk)
ISBN: 9781472447685 (pbk)
ISBN: 9781472447661 (ebk-PDF)
ISBN: 9781472447678 (ebk-ePUB)
James Reason is Professor Emeritus of Psychology at the University of Manchester, England. He is consultant to numerous organizations throughout the world, sought after as a keynote speaker at international conferences and author of several renowned books including Human Error (CUP, 1990), Managing the Risks of Organizational Accidents (Ashgate, 1997), The Human Contribution (Ashgate, 2008) and A Life in Error (Ashgate, 2013).
Introduction
The term organizational accidents (shortened here to orgax) was coined in the early 1990s and was developed in the Ashgate book published in 1997 entitled Managing the Risks of Organizational Accidents. Sales of the book indicate that many people may have read it it remains Ashgates all-time best-selling book on human performance. So the present book is not a revision, but a revisit. A lot has happened in the ensuing 18 years, my aim here is to update and extend the arguments presented in the first book to accommodate these developments. In short, this book is an addition rather than a replacement. And enough has happened in the interim to require a separate book.
Despite their huge diversity, each organizational accident has at least three common features: hazards, failed defences and losses (damage to people, assets and the environment). Of these, the most promising for effective prevention are the failed defences. Defences, barriers, safeguards and controls exist at many levels of the system and take a large variety of forms. But each defence serves one or more of the following functions:
to create understanding and awareness of the local hazards;
to give guidance on how to operate safely;
to provide alarms and warnings when danger is imminent;
to interpose barriers between the hazards and the potential losses;
to restore the system to a safe state after an event;
to contain and eliminate the hazards should they escape the barriers and controls;
to provide the means of escape and rescue should the defences fail catastrophically.
) to be reconsidered later.
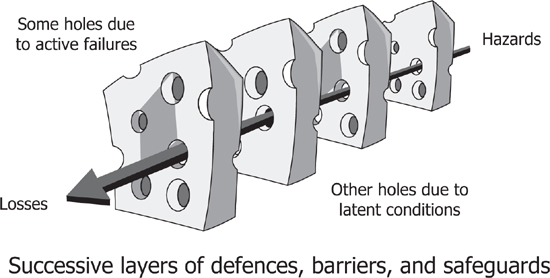
Figure 1.1 The Swiss cheese model of accident causation
The gaps in the defences arise for two reasons active failures and latent conditions occurring either singly or in diabolical combinations. They are devilish because in some cases the trajectory of accident liability need only exist for a very short time, sometimes only a few seconds:
Active failures: these are unsafe acts errors and/or procedural violations on the part of those in direct contact with the system (sharp-enders). They can create weaknesses in or among the protective layers.
Latent conditions: in earlier versions of the Swiss cheese model (SCM), these gaps were attributed to latent failures. But there need be no failure involved, though there often is. A condition is not necessarily a cause, but something whose presence is necessary for a cause to have an effect like oxygen is a necessary condition for fire, though an ignition source is the direct cause.
Designers, builders, maintainers and managers unwittingly seed latent conditions into the system. These arise because it is impossible to foresee all possible event scenarios. Latent conditions act like resident pathogens that combine with local triggers to open up an event trajectory through the defences so that hazards come into harmful contact with people, assets or the environment. In order for this to happen, there needs to be a lining-up of the gaps and weaknesses creating a clear path through the defences. Such line-ups are a defining feature of orgax in which the contributing factors arise at many levels of the system the workplace, the organization and the regulatory environment and subsequently combine in often unforeseen and unforeseeable ways to allow the occurrence of an adverse event. In well-defended systems, such as commercial aircraft and nuclear power plants, such concatenations are very rare. This is not always the case in healthcare, where those in direct contact with patients are the last people to be able to thwart an accident sequence.
Latent conditions possess two important properties: first, their effects are usually longer lasting than those created by active failures; and, second, they are present within the system prior to an adverse event and can in theory at least be detected and repaired before they cause harm. As such, they represent a suitable target for safety management. But prior detection is no easy thing because it is very difficult to foresee all the subtle ways in which latent conditions can combine to produce an accident.
It is very rare for unsafe acts alone to cause such an accident where this appears to be the case, there is almost always a systemic causal history. An obvious domain where unsafe acts might be the sole factor is healthcare where the carer appears to be the last line of defence. Three healthcare case studies are among the 10 discussed below. In each, the unsafe actions of the immediate carers are shaped, even provoked, by systemic factors.
Promising candidates for close study are the generic organizational processes that exist in all systems regardless of domain designing, building, operating, managing, maintaining, scheduling, budgeting, communicating and the like.
This book extends and develops these ideas using case studies that have occurred in a variety of domains in the period that has passed since the 1997 book was written and published. These analyses provide the raw data for the process of drilling down into the underlying causal pathways. Many contributing latent conditions recur in a variety of domains. A number of these organizational issues, design, procedures and communications in particular are examined in detail in order to reveal likely problems before they combine to penetrate the defences-in-depth.
Font size:
Interval:
Bookmark:
Similar books «Organizational Accidents Revisited»
Look at similar books to Organizational Accidents Revisited. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Organizational Accidents Revisited and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.