Mary Courtney - Using Evidence to Guide Nursing Practice
Here you can read online Mary Courtney - Using Evidence to Guide Nursing Practice full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2009, publisher: Churchill Livingstone, genre: Politics. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Using Evidence to Guide Nursing Practice
- Author:
- Publisher:Churchill Livingstone
- Genre:
- Year:2009
- Rating:3 / 5
- Favourites:Add to favourites
- Your mark:
Using Evidence to Guide Nursing Practice: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Using Evidence to Guide Nursing Practice" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Using Evidence to Guide Nursing Practice 2e is an invaluable how-to guide for students and experienced nurses alike. Emphasis is placed on how to develop an evidence-based culture in the workplace, support clinicians to make decisions using the best available evidence and translating this evidence into practice. This new edition is divided into five concise sections which guide readers from an examination of evidence, to developing a workplace culture that supports Evidence-Based Practice. It demonstrates how to locate and appraise evidence, how to evaluate practice and finally how to translate evidence into practice with a new applied case study included.
- includes two new chapters; Locating and appraising the evidence and Evidence to inform nursing practice: An applied approach
- highlights Evidence-based Practice (EBP) initiatives and demonstrates how to develop an evidence-based culture in the workplace
- includes Step-by-step guides to undertaking a systematic review, a clinical audit and a program evaluation
- each chapter will have contributions from experienced academics and clinicians across Australia so as to ensure health industry relevance and academic rigour are addressed
Mary Courtney: author's other books
Who wrote Using Evidence to Guide Nursing Practice? Find out the surname, the name of the author of the book and a list of all author's works by series.





Using Evidence to Guide Nursing Practice — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Using Evidence to Guide Nursing Practice" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
PART ONE
INTRODUCTION
PART TWO
DEVELOPING AN EVIDENCE-BASED CULTURE
PART THREE
LOCATING THE EVIDENCE
PART FOUR
HOW TO EVALUATE CLINICAL PRACTICE
PART FIVE
TRANSLATING EVIDENCE INTO PRACTICE
USING EVIDENCE TO GUIDE NURSING PRACTICE
2e
Mary Courtney
Helen McCutcheon
CHURCHILL LIVINGSTONE
CHAPTER 1 Evidence-based nursing practice
Mary Courtney, Claire Rickard, Joy Vickerstaff, Anthea Court
1.1 Learning objectives
After reading this chapter, you should be able to:
This chapter introduces the reader to the development of the evidence-based practice (EBP) movement and provides an overview of why EBP has spread so rapidly over the past 15 years. It explains how evidence may be incorporated into nursing practice and examines the challenges the EBP-based movement has posed for both nursing education and nursing research.
Health professionals currently advise their patients to stop smoking. Why do they give this advice? Why dont they advise them to start smoking or increase their smoking intake? The reason is that evidence is available which demonstrates:
This is an example of evidence that can identify the cause of a disease and the effectiveness of an intervention to improve patient outcomes and decrease illness and disability.
).
).
:2) published the first textbook on evidence-based medicine and defined it as:
The conscientious, explicit and judicious use of current best evidence in making decisions about the healthcare of patients.
also included patient values as well as clinical expertise:
The practice integrates clinical expertise and patient values with the best available research evidence.
).
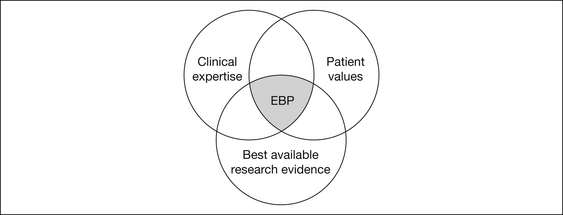
Figure 1.1 The three elements of evidence-based practice
Source:
).
There are benefits of EBP for patients/consumers, nurses, healthcare organisations and the community.
To healthcare consumers, it may seem ludicrous, or even frightening, that the EBP concept is relatively new. Patients typically accept recommended care from health professionals with the unspoken assumption that the practitioner knows what works.
In an ideal world, nurses could keep up to date by reading all of the published literature in their relevant area. In reality, with approximately a thousand new publications each year relevant just to surgical nursing, for example, this is clearly an impossible task. EBP allows a more structured and streamlined way of keeping abreast of relevant new developments without becoming overwhelmed by information overload.
EBP also allows nurses to communicate effectively with their patients and with the healthcare team about the rationales for decision making and care plans. An EBP nurse is a confident professional, feeling assured that they are providing care which is supported by facts rather than habits, and can take legal accountability for their practice.
A commitment to EBP philosophy allows healthcare organisations to position themselves in the market as quality institutions. An EBP-compliant institution should be less likely to attract litigation, and will be able to successfully defend the care delivered if it was in line with international best evidence at the time of care. In addition, EBP allows the scrutinising of practice for effectiveness. This process often results in practice changes that allow significant cost savings, or alternatively justify necessary additional expenditure. This is attractive to organisations frequently struggling to meet assigned budgetary limits, or lobbying government for additional funds.
Through the utilisation of EBP, finite resources are not wasted on the delivery of ineffective interventions. Additionally, EBP limits the amount of disability and suffering throughout the community by ensuring the most current and effective care is provided.
You may be wondering how nurses made decisions about their practice before the relatively recent EBP movement, or even what the alternatives to EBP are. If we are honest, for most of our working life we function on automatic pilot; that is, we ritualistically do things the way we have always done them, the way we were taught as a student or graduate nurse, or just in the accepted way of doing things in our current workplace.
However, at times our comfort zone is challenged, and we identify a knowledge deficit when confronting an unusual or challenging problem. At times like these, practitioners may guide their practice by asking the opinion of colleagues or senior practitioners, reviewing employer policies, reading textbooks or lecture notes, leafing through nursing or other journals, and listening to speakers at professional conferences or other education forums. Can you think of some benefits and limitations to these methods of guiding practice? For example, if a decision needs to be made immediately, guidance from an experienced colleague or organisational manual provides a quick and easy reference tool. However, on the downside, even well-meaning and senior practitioners may not have the latest knowledge, and policy manuals are frequently out-of-date, even if they were prepared using the best evidence at the time of policy development.
for the spread of the EBP movement have been the:
However, health departments around the world are increasingly being stretched to cover ever-rising health expenditures and, with treatment and care costs increasing all the time, governments need to ensure they are using public funds for treatment and care that is effective with positive health outcomes and benefits for the public.
).
While EBP was initially limited to the practice of medicine it became clear that unless all the members of the health team embraced EBP it would have limited impact.
Evidence for practice decisions is increasingly available in online format. Some resources are available free of charge, while others attract a fee for use, although staff and students of healthcare facilities and universities can usually access these through the institution at no personal cost. Many electronic resources now provide links to full-text journal articles for some records. New products are constantly being developed to allow practitioners to quickly and easily search for relevant evidence. Some of the currently well-established and recommended sources of evidence are described below.
Font size:
Interval:
Bookmark:
Similar books «Using Evidence to Guide Nursing Practice»
Look at similar books to Using Evidence to Guide Nursing Practice. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Using Evidence to Guide Nursing Practice and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.