Pinal Francisco del - Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book
Here you can read online Pinal Francisco del - Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2019, publisher: Thieme Medical Publishing Inc., genre: Science. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.
- Book:Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book
- Author:
- Publisher:Thieme Medical Publishing Inc.
- Genre:
- Year:2019
- Rating:3 / 5
- Favourites:Add to favourites
- Your mark:
Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Pinal Francisco del: author's other books
Who wrote Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book? Find out the surname, the name of the author of the book and a list of all author's works by series.


Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Simon MacLean, Gregory Bain
Abstract
This chapter discusses the importance of the anatomy of distal radius in relation to fracture. First, we describe the microanatomy of the distal radius. Its microanatomy resembles that seen in everyday engineering structures; the subchondral bone plate and arrangement of trabeculae enabling the wrist to handle high multidirectional loads. Stability of the wrist is achieved by multiple ligamentous rings that confer stability within and between the rows and columns of the wrist. Ligamentous insertions play an important role in fracture morphology, both initiation and propagation of the fracture lines.
Hand position at impact determines the position of the carpus on the distal radius. When a line of differential load occurs in the scapholunate interval, scapholunate ligament injury (SLI) may result. SLI is associated with specific fracture types. Unmasking with scapholunate diastasis occurs when there is compromise to the secondary stabilizers.
The volar marginal rim fracture represents an important subset of fractures. These are associated with a higher rate of carpal ligamentous injury and fixation failure. Distal radius plate design has evolved to attempt to capture this fragment.
Lastly, we present a biomechanical model for distal radius fracture.
Keywords: distal radius fracture, microstructure, scapholunate injury, volar rim fracture, radiocarpal ligaments
Distal radius fractures (DRFs) are one of the most commonly treated injuries in orthopaedic practice. A bimodal distribution exists; in younger patients, caused by high-energy and in older patients, caused by low-energy falls. Osteoporotic DRFs reflect a change in the microarchitecture of the distal radius with aging and are a predictor for subsequent fracture of long bones. Classification systems have attempted to provide clarity to the morphology and treatment of these injuries.
With an improved understanding of the anatomy of distal radius, we are better equipped to treat the patient, respecting not just the fracture components but also the contribution of the surrounding ligaments, carpal bones, and other associated injuries. This chapter will explore the importance of each component and its interaction in the mechanism of fracture. First, we will study the microanatomy of the distal radius; and then we will focus on fracture initiation and the role of the carpus; and third, the role of the carpal ligaments and fracture propagation. We will look at the specific anatomy of the volar rim fracture. We will propose a biomechanical model for DRF.
Singh reported the trabecular structure of the proximal femur and changed our approach to the understanding and management of these injuries. and found it resembled many of the engineering concepts in everyday man-made structures. Interestingly, an engineer once advised us that he knew when he had the design correct and when it resembled the structures identified in nature.
The subchondral bone plate is a 2-mm-thick multilaminar plate that absorbs impact and transmits the load to the radial metaphysis. The superficial primary bone plate bridges the entire articular margin. Multiple deeper layers resemble a leaf spring used in the suspension of heavy motor vehicles.
Between these laminae, and connecting them, lie intralaminar struts. These are initially perpendicular to the joint line, but more proximally align with the radial shaft. Voids between the struts and laminae absorb impact and enable vessels to perforate. The struts between the laminae are mini I-beams, which make the structure strong but still enable it to bend. Engineers refer to this multilayered lamina construct as a honeycomb sandwich panel.
With physiological wrist extension, the volar capsule becomes taut, and the scaphoid and lunate load the distal radius subchondral bone plate.
The multilayered subchondral bone plate resists buckling and transmits the load to the intermediate trabeculae and then the metaphyseal arches ().
On a magnified view, areas can be seen where these trabeculae coalesce to form a rod and extend as longitudinal ridges down the diaphysis (), and prevent torsional failure and buckling.
The load bearing area of the lunate is very volar. The sagittal images demonstrate the thick volar trabecular columns spanning to the volar cortex of the metaphyseal radius (). This explains the devastating effect of Barton volar lip fracture, as the carpus will simply dislocate volarly.
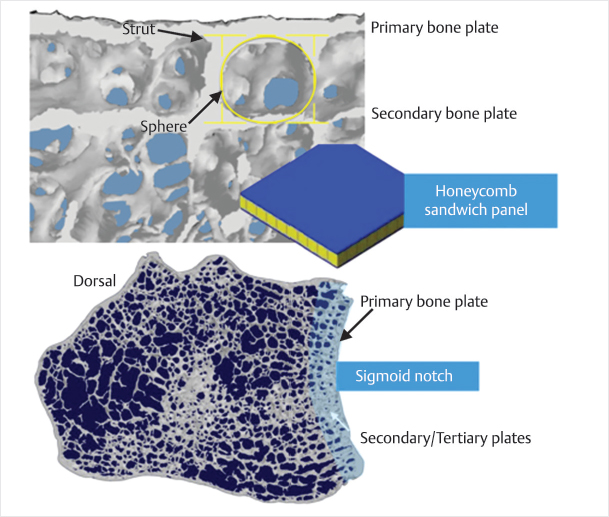
Fig. 1.1 Anatomy of the subchondral bone plate of the distal radius.
(Copyright Gregory Bain, MD)
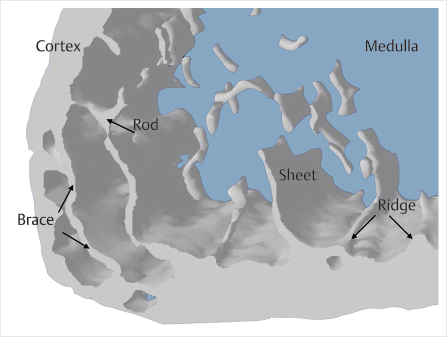
Fig. 1.2 The radial styloid cortex is quite thin but is reinforced by bracing trabeculae. The trabeculae are thin sheets of bone, which are designed to transmit load. There the sheets meet and coalesce into rods, which then become the ridges on the endosteal cortex.
(Copyright Gregory Bain, MD)
Further dorsal on the lunate facet, trabeculae course dorsally forming a curve in the shape of a gothic arch, with an underlying intramedullary vault. From medial to lateral through the distal radius, these gothic arches are in seriesconnected by interarch struts. In normal bone under normal loads, the parabolic shape of the arch transfers loads in a longitudinal and lateral direction, to the base of the arch without creating tension ().
At the base of each arch, the trabeculae merge with the cortex, which then becomes thickenedtherefore buttressing the arch. In contrast, at the articular margin, the cortex is thin. It acts to suspend the subchondral bone plate and serves as a site for ligament attachment, rather than to bear the load.
The microstructure of the distal radius resembles an arch bridge with the following equivalent: deckSBP, intermediate strutsintermediate trabeculae, archesarches, and bridge foundationcortex. The deck is a tightly held lattice with multiple I-beams in a multilayer sandwich panel construct. This resists buckling, absorbs impact, and takes the entire load ().
The arches and intermediate struts are a semiflexible construct, which distributes compressive forces from the deck to the base (diaphysis). The orientation of the microstructure ensures that forces are distributed in compression rather than tension (where the bone is weakest).
Force transfer from the hand to the radius at the time of DRF involves the transmission of force through the three columns of the wrist. The three columns are bound by a series of ligamentous rings. These ligamentous rings provide stability within and between the proximal and distal rows of the wrist ().
The distal radioulnar joint is bound by a fibroligamentous ring. Disruption of this at the time of DRF can lead to dislocation of this joint and distal radioulnar instability, if not addressed at the time of surgery.
Within the proximal carpal row, interosseous ligaments on the volar and dorsal aspects of the scapholunate and lunotriquetral joints form a ring. Transmission of force from the central column to the scaphoid, lunate, or both can lead to a disruption of these ligaments and a greater arc injury or an impaction fracture of the distal radius.
Font size:
Interval:
Bookmark:
Similar books «Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book»
Look at similar books to Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Distal Radius Fractures and Carpal Instabilities: FESSH IFSSH 2019 Instructional Book and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.