David Hawkins - The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools
Here you can read online David Hawkins - The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2019, publisher: Foundation for Critical Thinking, genre: Children. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools
- Author:
- Publisher:Foundation for Critical Thinking
- Genre:
- Year:2019
- Rating:5 / 5
- Favourites:Add to favourites
- Your mark:
The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
David Hawkins: author's other books
Who wrote The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools? Find out the surname, the name of the author of the book and a list of all author's works by series.

The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:

 Copyright 2010 Foundation for Critical Thinking
Copyright 2010 Foundation for Critical Thinking
Foundation for Critical Thinking Press
707-878-9100
www.criticalthinking.org
All rights reserved. No part of this guide may be reproduced, in any form or by any means, without permission in writing from the Foundation for Critical Thinking, except for the quotation of brief passages in criticism.
Printed in the United States of America.
ISBN 978-0-944583-42-5
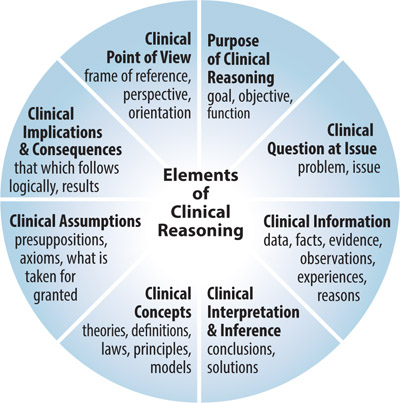
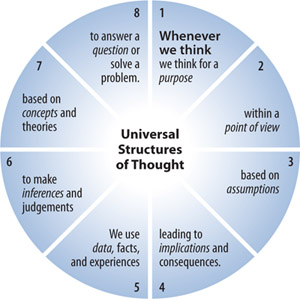
The elements of clinical reasoning that appear in the diagram below provide the basis for analyzing the structures present in all thinking. Whenever we think, we think for a purpose within a point of view based on assumptions leading to implications and consequences. We use concepts, ideas, and theories to interpret data, facts, and experiences in order to answer questions, solve problems, and resolve issues.
Each of these structures has implications for the others. If you change your purpose, for example, you change your questions and problems. You are then forced to seek new information and data. And this changes the implications and consequences of your conclusions and decisions.

- Can you state your purpose clearly?
- What is the objective of your clinical reasoning?
- Does your reasoning focus throughout on your clinical goal?
- Is your clinical goal realistic?
- What clinical question are you trying to answer?
- Are there other ways to think about the question?
- Can you divide the question into sub-questions?
- Is this a question that has one right answer or can there be more than one reasonable answer?
- Does this question require clinical judgment rather than facts alone?
- What assumptions are you making? Are they justified?
- How are your assumptions shaping your point of view?
- Which of your assumptions might reasonably be questioned?
- What is your point of view? What insights is it based on? What are its weaknesses?
- What other points of view should be considered in reasoning through this problem? What are the strengths and weaknesses of these viewpoints? Are you fairmindedly considering the insights behind these viewpoints?
- To what extent is your reasoning supported by relevant data?
- Do the data suggest explanations that differ from those you have given?
- How clear, accurate, and relevant are the data to the clinical question at issue?
- Have you gathered data sufficient to reach a valid conclusion?
- What key concepts and theories are guiding your clinical reasoning?
- What alternative explanations might be possible, given these concepts and theories?
- Are you clear and precise in using clinical concepts and theories in your reasoning?
- Are you distorting ideas to fit your agenda?
- To what extent do the data support your clinical conclusions?
- Are your inferences consistent with each other?
- Are there other reasonable inferences that should be considered?
- What implications and consequences follow from your reasoning?
- If we accept your line of reasoning, what implications or consequences are likely?
- What other implications or consequences are possible or probable?
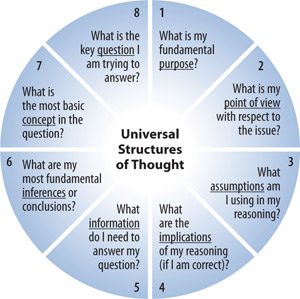
Note: When we understand the structures of thought, we ask important questions implied by these structures.
A 53 year old man complains of severe pain in his left big toe for the past 2 days. The patient has a past medical history of two episodes of acute gouty arthritis in the past 3 months, hypertension for 10 years, and dyslipidemia. He is currently receiving a thiazide diuretic for his high blood pressure, atrovastatin for his high cholesterol, and one aspirin tablet daily to prevent heart attacks. Laboratory studies revealed a serum urate concentration of 10mg/dL and a very high urinary urate concentration. The patients blood pressure is 130/80 mmHg. A positive diagnosis of acute gouty arthritis was confirmed by taking a sample of the patients synovial fluid taken from the affected joint and examining it under a polarizing microscope.
To treat the acute attack and to prevent recurrent attacks.
- 1.What is the most effective way to treat this patients acute attack?
- 2.What is the most effective way to prevent recurrent attacks in this patient?
- 3.What adjustments, if any, need to be made to this patients other medications?
- 1.Colchicine will not work in this case.
- 2.Baby aspirin will not significantly increase serum urate concentrations.
- 3.Traditional medicine has the best answers in a case like this, so we dont need to consider alternative therapies.
- 1.A conservative approach would be to treat the acute attack and discontinue the thiazide diuretic because it increases serum uric acid concentration and therefore the propensity for recurrent attacks.
- 2.A more aggressive approach would be to initiate preventive therapy irrespective of the decision to continue or discontinue the diuretic.
- 1.Either colchicine or a non-steroidal anti-inflammatory agent can be used to treat acute attacks.
- 2.Colchicines effectiveness diminishes 48 hours after onset of pain.
- 3.Either probenecid or allopurinol can be used to prevent recurrent attacks.
- 4.Probencid increases urinary uric acid excretion.
Font size:
Interval:
Bookmark:
Similar books «The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools»
Look at similar books to The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book The Thinkers Guide to Clinical Reasoning: Based on Critical Thinking Concepts and Tools and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.