Ultrasound
Sonography has become an important part of the pediatric imaging armamentarium perhaps the most important. Its strengths are many. To begin with, it does not use ionizing radiation. In addition ultrasound does not require the administration of intravenous contrast agents; although several ultrasound contrast agents have been recently developed that can increase the accuracy of the imaging examination []. Furthermore sedation is very rarely required.
The most common indications for sonographic imaging of the kidneys include: urinary tract infection [], and assessment for possible urinary obstruction. Ultrasound can also assess other findings noted on antenatal imaging such as renal agenesis, ectopia, dysplasia or mass.
The ultrasound examination can be tailored in many ways to suit the patient and clinical situation. A patient who is upset or frightened can be scanned lying next to a parent or in the arms of a parent, which can alleviate some anxiety. Coupled with a calm and reassuring environment and various distractions (e.g., toys, music, videos, computer tablets), this setting often allows for the performance of a satisfactory diagnostic study. The need for sedation is extremely rare but may be considered on a case-by-case basis.
The patient can be scanned in various positions (supine, prone, decubitus) depending on the scenario. In fact altering position can at times be helpful particularly in determining if a structure such as a calculus is mobile. In some situations the ultrasound examination can be repeated after an intervention has been performed in order to determine whether it was successful or resulted in a complication. One can study the urinary tract prior to or after voiding, after placement of a bladder catheter, ureteral stent or nephrostomy catheter or after biopsy. These repeated examinations can be done without concern for the effects of radiation.
By and large the small body habitus of children allows for excellent sonographic imaging of the urinary tract. There are cases of larger teenagers and obese children in which sonography of the urinary system can be suboptimal. Scanning of the kidneys is performed mainly with curved array transducers for assessment of kidney length, status of the renal parenchyma, the pelvocaliceal system, ureters and the bladder. These images can be supplemented with those obtained with a high-resolution linear transducer, which offers a superior level of spatial resolution but is limited in terms of the depth to which the transducer can penetrate. For that reason high resolution sonography is particularly well suited to neonates, infants and younger children. In older children, the distance between the transducer and the kidneys may preclude this type of higher resolution examination.
The kidneys are ovoid organs that typically lie in the retroperitoneal renal fossae, although they can be ectopic. Their lengths can be measured and compared with published nomograms [].
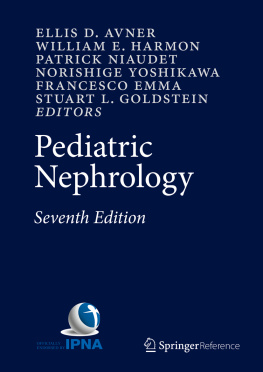
Fig. 1.1
Nomograms delineate the predicted mean and 95 % prediction limits of renal length as a function of age ( a ), height ( b ), weight ( c ), and total body surface area ( d )
In healthy children there is a difference in echogenicity between normal renal cortex and the medullary pyramids, with the former more echogenic and the latter more hypoechoic (Fig. ]. In addition, there may be lobulation of the renal outline, especially in neonates. This should not be confused with scarring. The notching of normal lobulation tends to be seen in the portion of the cortex between pyramids; whereas focal scarring tends to occur in portions of the cortex directly overlying the pyramid.
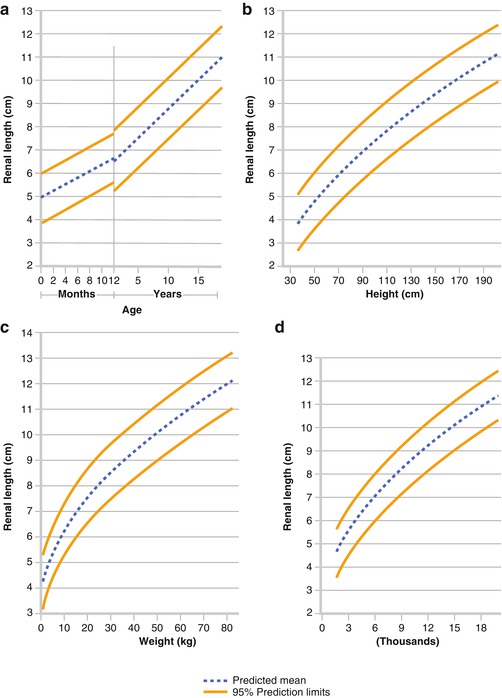
Fig. 1.2
Ultrasound of the normal kidney (length outlined with calipers) demonstrates renal pyramids which are nearly anechoic ( arrows ) and which can be mistaken for dilatation of the renal collecting system
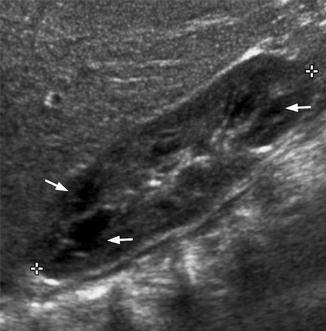
Fig. 1.3
Ultrasound of the normal neonatal kidney in which the renal cortex is more echogenic than the adjacent liver. This can be a normal finding in the neonate. After several months the renal cortex should be less echogenic than the liver
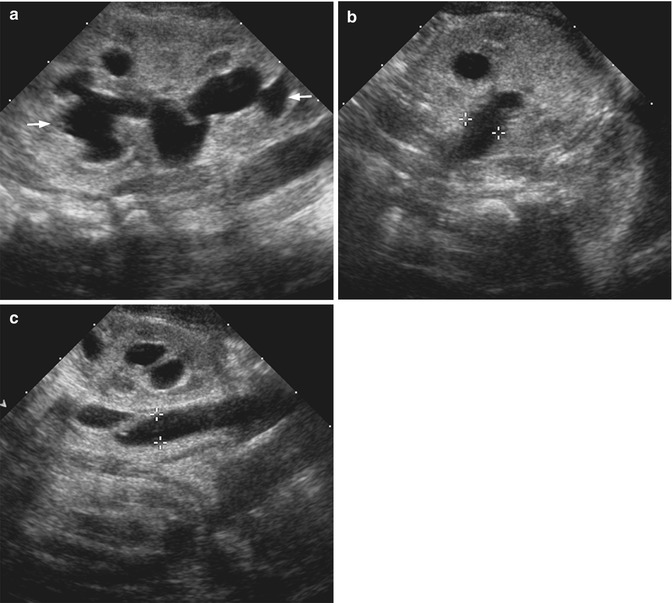
The degree of renal collecting system dilatation can be assessed both qualitatively and quantitatively. Measurement of pelvic dilatation can be assessed at the level of the renal hilum or just beyond it in the case of an extrarenal pelvis. A full bladder can exaggerate the degree of dilatation. It therefore may be prudent to assess the pelvic diameter after voiding if the urinary bladder is over-distended. If the ureter is dilated, its diameter can be assessed along its course, although it can be visualized most reliably proximally and distally (Fig. ]. The degree of obstruction caused by a calculus can also be assessed with sonography.
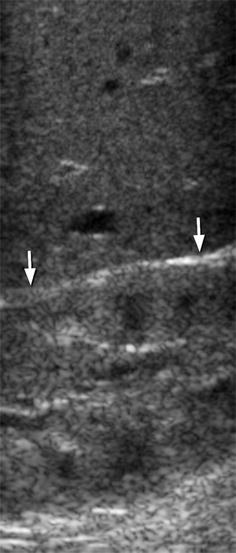
Fig. 1.4
( a ) Ultrasound of the kidney in the longitudinal plane demonstrates moderate pelvocaliceal dilatation ( arrows ). ( b ) In the transverse plane the renal pelvis is measured with respect to its maximal AP diameter (calipers). ( c ) Scanning along the flank, one can often visualize the ureter if it is dilated (calipers)
Colour Doppler and pulsed Doppler interrogation of the kidneys can be used to assess vascularity of the kidneys. The study can assess the vessels from the ostia of the main renal arteries and veins through the arcuate vessels in the renal parenchyma. Indications for Doppler evaluation include suspicion of renal arterial or venous thrombosis [].
Voiding Cystourethrography
Voiding cystourethrography is the study of choice for diagnosing vesicoureteral reflux and assessing the anatomy of the bladder and urethra. Indications for this investigation include urinary tract infection []. This latter method, termed cyclic VCUG , has demonstrated greater sensitivity in detecting reflux, but results in a higher radiation dose than does the single cycle method.