Pamela R. Roberts - Comprehensive Critical Care: Adult
Here you can read online Pamela R. Roberts - Comprehensive Critical Care: Adult full text of the book (entire story) in english for free. Download pdf and epub, get meaning, cover and reviews about this ebook. year: 2017, publisher: Society of Critical Care Medicine, genre: Science. Description of the work, (preface) as well as reviews are available. Best literature library LitArk.com created for fans of good reading and offers a wide selection of genres:
Romance novel
Science fiction
Adventure
Detective
Science
History
Home and family
Prose
Art
Politics
Computer
Non-fiction
Religion
Business
Children
Humor
Choose a favorite category and find really read worthwhile books. Enjoy immersion in the world of imagination, feel the emotions of the characters or learn something new for yourself, make an fascinating discovery.

- Book:Comprehensive Critical Care: Adult
- Author:
- Publisher:Society of Critical Care Medicine
- Genre:
- Year:2017
- Rating:5 / 5
- Favourites:Add to favourites
- Your mark:
Comprehensive Critical Care: Adult: summary, description and annotation
We offer to read an annotation, description, summary or preface (depends on what the author of the book "Comprehensive Critical Care: Adult" wrote himself). If you haven't found the necessary information about the book — write in the comments, we will try to find it.
Neurologic Critical Care
Cardiovascular Critical Care
Respiratory Critical Care
Critical Care Infectious Disease
Hepatic, Gastrointestinal, and Hematologic/Oncologic Disease in the ICU
Renal and Metabolic Disorders in the ICU
Environmental and ToxicologicInjury
Pharmacologic Issues in the ICU
Surgical and Obstetrical Critical Care
Administrative and Ethical Issues in the Critically Ill
This new resource includes up-to-date information on the full gamut of critical care topics, with dozens of charts and tables to aid study and suggested to guide further exploration.
Pamela R. Roberts: author's other books
Who wrote Comprehensive Critical Care: Adult? Find out the surname, the name of the author of the book and a list of all author's works by series.


Comprehensive Critical Care: Adult — read online for free the complete book (whole text) full work
Below is the text of the book, divided by pages. System saving the place of the last page read, allows you to conveniently read the book "Comprehensive Critical Care: Adult" online for free, without having to search again every time where you left off. Put a bookmark, and you can go to the page where you finished reading at any time.
Font size:
Interval:
Bookmark:
Part 1: Neurological Critical Care
Stuart McGrane, MBChB, MSCI, Pratik P. Pandharipande, MD, MSCI, and Christopher G. Hughes, MD
Fred Rincon, MD, MSc, MBE, FACP, FCCP, FCCM
Scott A. Marshall, MD, and Geoffrey S. F. Ling, MD, PhD, FAAN
Sherry H-Y. Chou, MD, MMSc, FNCS
Part 2: Cardiovascular Critical Care
Antoinette Spevetz, MD, FCCM, FACP, and Joseph E. Parrillo, MD, FACC, MCCM
Michael R. Pinsky, MD, CM, Dr h.c., FCCP, MCCM
Felix Y. Lui, MD, and Kimberly A. Davis, MD, MBA
Chapter 8: Severe Heart Failure, Cardiogenic Shock, and Pericardial Tamponade
(Including Principles of Intra-aortic Balloon Pumps and Ventricular Assist Devices)
Etienne Gayat, MD, PhD, and Alexandre Mebazaa, MD, PhD
Sachin Yende, MD, MS, David T. Huang, MD, MPH, and R. Phillip Dellinger, MD, MCCM
Deepa M. Patel, MD, and Craig M. Coopersmith, MD
Fredric Ginsberg, MD, FACC, FCCP, and Joseph E. Parrillo, MD, FACC, MCCM
Ravi Agarwala, MD, FRCPC, Sean Patrick Whalen, MD, and Natalie Bradford, MD
Chapter 13: Valvular Heart Disease, Acute Aortic Dissection, and Patient Care
After Cardiac Surgery
Michael H. Wall, MD, FCCM, and Pamela R. Roberts, MD, FCCM
Amanda M. Gomes, MD
Marcos Emanuel Gomes, MD, and Pamela R. Roberts, MD, FCCM, FCCP
Stylianos Voulgarelis, MD, and Sylvia Y. Dolinski, MD, FCCP
Part 3: Respiratory Critical Care
Nicholas C. Watson, MD, and Stephen O. Heard, MD
Eric Ursprung, MD, and Theofilos P. Matheos, MD
Debasree Banerjee, MD, MS, Jeffrey Mazer, MD, and Nicholas Ward, MD
Jennifer A. LaRosa, MD, FCCM, FCCP, and R. Phillip Dellinger, MD, MCCM
Neil R. MacIntyre, MD
Kenneth E. Wood, DO, and Jason A. Stamm, MD
Scott E. Kopec, MD, FCCP, and Marie T. Mullen, MD
Robert A. Balk, MD
Part 4: Critical Care Infectious Diseases
Ryo Yamamoto, MD, and Ramon F. Cestero, MD, FACS
Gourang Patel, PharmD, MSc, and Anand Kumar, MD
Gloria Vazquez-Grande, MD, and Anand Kumar, MD
Shravan Kethireddy, MD, Anna Chen, MD, Jonathan Perez, MD, and Mary Jane Reed, MD, FCCM
Part 5: Hepatic, Gastrointestinal, Hematologic/Oncologic Disease in the ICU
Vinod P. Balachandran, MD, and Soumitra R. Eachempati, MD, FACS, FCCM
Adil M. Abuzeid, MBBS, and Nabil M. Issa, MD
Mario Raul Villalba, MD, FACS, and Martin A. Schreiber, MD, FACS
John Crommett, MD, and Joseph L. Nates, MD, MBA, FCCM
Part 6: Renal and Metabolic Disorders in the ICU
Chapter 33: Acute and Chronic Renal Failure and Management (Including Hemodialysis and
Continuous Renal Replacement Therapies)
Michael L. Bentley, PharmD, FCCM, FCCP, FNAP, and Ashita J. Tolwani, MD, MSc
Alisha Bhatia, MD, and David M. Rothenberg, MD, FCCM
Linda L. Maerz, MD, FACS, FCCM
Gozde Demiralp, MD, and Pamela R. Roberts, MD, FCCM, FCCP
Nestor Arita, MD, Jeremy L. Ward, MD, and Paul E. Marik, MD, FCCM, FCCP
Pamela R. Roberts, MD, FCCM, FCCP
Part 7: Environmental and Toxicologic Injury
Todd Huzar, MD, and James M. Cross, MD, FACS
Michael Sirimaturos, PharmD, BCNSP, BCCCP, FCCM, Rebeca L. Halfon, BS, PharmD, and
Janice L. Zimmerman, MD, MCCM, FCCP
Janice L. Zimmerman, MD, MCCM, FCCP
Part 8: Pharmacologic Issues in the ICU
Quinn A. Czosnowski, PharmD, and Craig B. Whitman, PharmD, BCPS, BCCCP
Brian L. Erstad, PharmD, MCCM, and Courtney McKinney, PharmD
Part 9: Surgical and Obstetrical Critical Care
Yatin Mehta, MD, Jaya Sugunaraj, MD, Mark A. Kleman, DO, M. Camilla Bermudez, MD, Heather J. Johnson, PharmD, Patricio Andres Sanchez-Cueva, MD, and Mary Jane Reed, MD, FCCM
Sherry Sixta, MD, and Rosemary Kozar, MD, PhD
Christina C. Kao, MD, Tashinga Musonza, MD, Lillian S. Kao, MD, MS, and S. Rob Todd, MD
Jennifer E. Hofer, MD, Karen C. Patterson, MD, and Michael F. OConnor, MD, FCCM
Part 10: Administrative and Ethical Issues in the Critically Ill
Sara R. Gregg, MHA, and Timothy G. Buchman, MD, PhD, MCCM
Jean-Louis Vincent, MD, PhD, FCCM
Andrew M. Naidech, MD, MSPH
Fred Rincon, MD, MSc, MBE, FACP, FCCP, FCCM
Altered Mental Status During Critical Illness: Delirium and Coma
Stuart McGrane, MBChB, MSCI, Pratik P. Pandharipande, MD, MSCI, and Christopher G. Hughes, MD
Key words: delirium, coma, Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), Intensive Care Delirium Screening Checklist (ICDSC), Richmond Agitation-Sedation Scale (RASS)
Critically ill patients often manifest varying degrees of altered mental status secondary to their acute disease processes or as a consequence of the therapies used to treat disease. These mental status changes range from coma to hyperactive delirium. A comatose patient is unresponsive to physical or verbal stimuli, whereas delirium is an acute and fluctuating disorder of consciousness characterized by inattention, disorganized thinking, and perceptual disturbances ( Figure 1 ). Alterations in mental status have traditionally been considered expected consequences of critical illness, and clinicians are increasingly aware that these mental status changes are manifestations of acute brain organ dysfunction that are associated with worse clinical outcomes. Early studies evaluating coma and delirium were hampered by the many different terms (eg, confusional state, ICU psychosis, acute brain dysfunction , and encephalopathy ) used to describe altered mental status during critical illness. Additionally, the lack of validated bedside tools (besides the comprehensive Diagnostic and Statistical Manual of Mental Disorders ) to diagnose delirium prevented the incorporation of delirium monitoring into routine clinical care in the ICU.
Figure 1. Delineation between delirium and coma, highlighting the cardinal symptoms of delirium
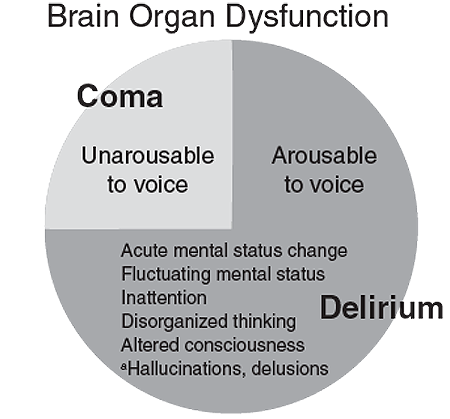
aOptional symptoms of delirium (may be present but are not required for the diagnosis of delirium).
DIAGNOSIS OF ACUTE BRAIN DYSFUNCTION
Traditionally, many scales have been available to assess the level of sedation and agitation in ICU patients, including the Ramsay scale, Riker Sedation-Agitation Scale (SAS), motor activity assessment scale, and Richmond Agitation-Sedation Scale (RASS). The recent guidelines on pain, agitation, and delirium from the Society of Critical Care Medicine recommend the use of the RASS and SAS due to their psychometric properties and validity in critically ill patients. The RASS ( Figure 2 ) also has been shown to detect variations in the patients level of consciousness over time or in response to changes in sedative and analgesic drug use. As a first step in assessing the level of consciousness, a sedation-agitation scale should be used. Patients who are unresponsive to verbal commands (eg, a RASS -4 or-5) are considered to be in a coma and cannot be evaluated for delirium at that time. Patients who are responsive to verbal stimuli (eg, RASS -3 and lighter) can further be evaluated for the content of that arousal via the use of delirium monitoring instruments.
Figure 2. The Richmond Agitation-Sedation Scale (RASS)
Score | Term | Description |
+4 | Combative | Overtly combative, violent, immediate danger to staff |
+3 | Very agitated | Pulls or removes tubes or catheters; aggressive |
+2 | Agitated | Frequent nonpurposeful movement, fights ventilator |
+1 | Restless | Anxious but movements not aggressive or vigorous |
Font size:
Interval:
Bookmark:
Similar books «Comprehensive Critical Care: Adult»
Look at similar books to Comprehensive Critical Care: Adult. We have selected literature similar in name and meaning in the hope of providing readers with more options to find new, interesting, not yet read works.
Discussion, reviews of the book Comprehensive Critical Care: Adult and just readers' own opinions. Leave your comments, write what you think about the work, its meaning or the main characters. Specify what exactly you liked and what you didn't like, and why you think so.