1. Introduction
This atlas was written taking into consideration the most common problems that are frequently encountered in young children.
Interceptive treatment is intervening in the developing dentition to allow it to achieve the best occlusion possible or to make subsequent treatment as simple and short as possible (DiBiase ).
There is no doubt that early treatment can be justified if it provides additional benefits to the patient.
The question of when, how, and why is answered in depth in all the clinical cases contained in this atlas. The goal is to focus on functional and skeletal rather than dental correction.
Knowing the diagnosis criteria and which type of cases should be treated early, will permit the clinician to offer the most efficient solution for each individual patient. In general the first phase of treatment in the early mixed dentition has to be followed by a second phase in the permanent dentition.
When and how much growth will occur is unpredictable in some patients, but the direction of growth can be managed (Sureh). However, it is important for the clinician to be able to diagnose and intercept certain developing problems through early treatment.
Many other cases should be supervised, but not treated until the permanent teeth are in place. We must base our decision on a correct diagnosis taking into account that the correction of functional and skeletal imbalances is fundamental before the eruption of all the permanent teeth.
One of the most important advantages to begin the treatment early is to take advantage that in early mixed dentition, the skeletal growth pattern can be modified to a certain point. Other doctors with different protocols suggest that the treatment has to begin after the eruption of the second molars (Behrents ). At this time growth modification will be limited.
Specific indications for early treatment include class II or class III malocclusion, with maxillary midface deficiency anterior and posterior crossbite (unilateral and bilateral), midline discrepancies due to early loss of deciduous teeth with a midline shift, severe anterior open bite, severe deep bite with palatal impingement, finger-sucking habits, crowding resulting in ectopic positioning of permanent teeth, etc. (Dugoni ).
But not all the circumstances are black or white; each patient is unique.
For example, the most appropriate timing for the treatment of class II malocclusion is controversial (Cozzani et al. ). Some clinicians advocate starting a first phase in mixed or temporary dentition, but others prefer to wait until the second molars were erupted.
Also, the timing of treatment interventions can be influenced by the severity of the malocclusion, the age, and maturity of the patient at the time the treatment begins.
It is important to emphasize that different types of brackets and wires were used by the authors to treat the patients since there isnt a single type of bracket or wire that performs a correct diagnosis in each clinical case, until now.
The role of the orthodontist is to manage the problem in the most efficient way for a better diagnosis. It is fully recognized that some malocclusions are best treated early for biological, functional, and social reasons.
Different alternatives for each malocclusion will be described step by step in each chapter.
It is evident that to design an efficient treatment plan, the clinician must understand the growth and development process very clearly.
It is well known that the difference in the response of patients with the same orthodontic treatment is the result of variability in the direction and rate of craniofacial growth.
It is impossible to decide the best time to begin the treatment based solely on the chronological age since the majority of the malocclusions that have to be treated during mixed dentition are the result of multiple factors.
In general mixed dentition is the best time to start treatment when the correction of habits with or without anterior or lateral transverse crossbite is indicated.
A panoramic radiograph is mandatory at age 810 years to confirm the presence or absence of agenesias, supernumerary teeth, cysts, mesiodens, etc.
The last chapter Controversies analyzes the most common ones in depth.
The following examples show the importance of the timing of treatment according to the initial pathology, the direction of growth, and the normalization of the functional problems such as nasal breathing and tongue posture at rest or during swallowing.
Although they were skeletal and dental class III at the beginning of the treatment with a similar biotype, the results that were achieved in the long term were completely different.
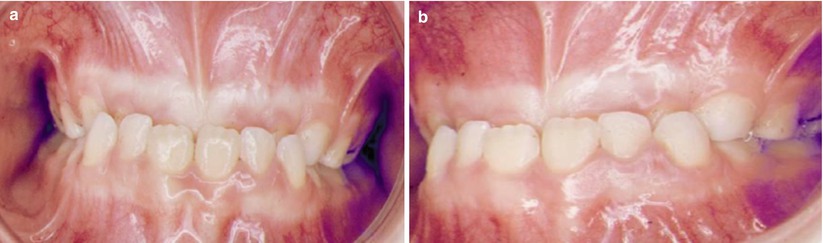
The parents of this 6-year-old patient asked for a second opinion about the best time to begin his treatment. They were very interested in having him treated very early and avoid the orthognathic procedure that was suggested. The front photographs confirmed a significant negative overjet and overbite that was present in the anterior region (Fig. a, b).
From the etiological point of view, it is important to consider that his two older sisters had class I molar and canine, but two of his seven cousins were class III and were treated with orthognathic surgery.
The dental front and lateral photographs showed that the lower incisors were in contact with the upper labial gingival tissues, and, until then and for unknown reasons, he only ate soft meals.
Fig. 1.1
( a , b ) Frontal and lateral pretreatment photographs. A significant negative overbite was present
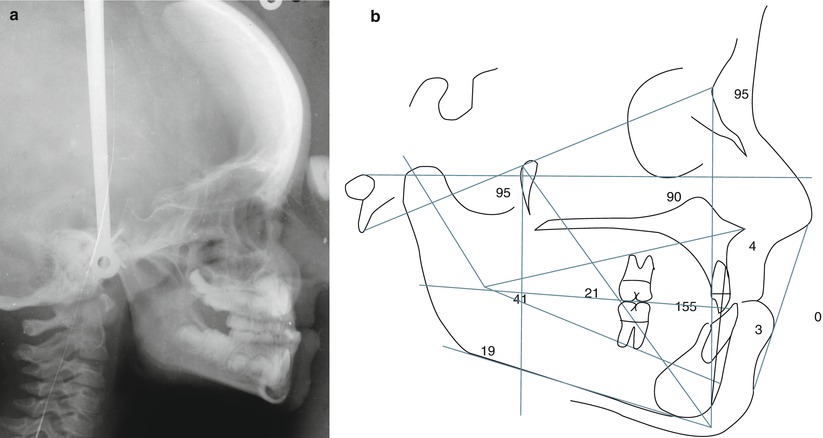
The lateral radiograph confirmed the negative anterior position of the front teeth. Ricketts analysis demonstrated normal convexity with a retruded upper lip and everted lower lip. An increased facial axis was present (95), along with a short lower anterior height (41) (Fig. a, b).
Fig. 1.2
( a , b ) Pretreatment lateral radiograph and Ricketts analysis
The real question is when would be the best treatment time to begin the correction of this Class III malocclusion? Is it advisable to begin now or to wait until 1112 or 18 years of age?
There is no doubt that the normalization of the anterior negative crossbite should take place as early as possible since it will help achieve a normal development of the maxilla and to improve the soft tissue profile.
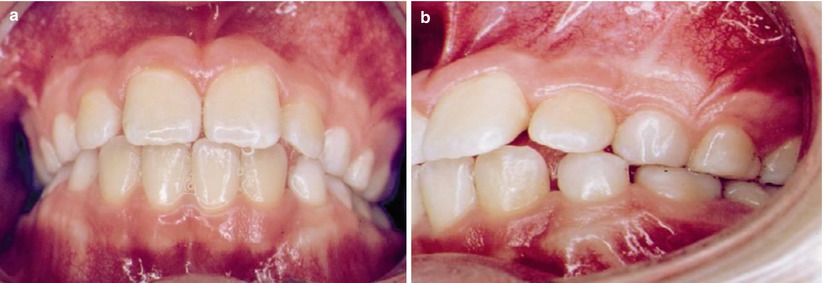
These were the results after 26 months with a functional appliance (Fig. a, b). Overjet and overbite were improved and midlines were almost normal. The objectives of phase I of treatment were accomplished. It was important to improve the anterior position of the tongue.
Fig. 1.3
( a , b ) Frontal and lateral posttreatment photographs at the end of phase I of treatment